Perhaps people have expected me to say more about the goings on in Congress lately. I have largely abstained because I don't have time to read 1,200 page draft bills, which means I have to depend on what other people say about them, which is inevitably tendentious, and you can read those folks as well as I can.
Also, my own position could not be more clear. Whatever comes out of this legislative session is barely going to begin to solve our problems, at best. While it's a worthy objective to get more people covered by health insurance, and the general idea of enforcing community rating and everybody into the pool is part of what a decent system will have to include, by itself it's not enough to be good or bad. It all depends on other pieces, which for the most part are not there.
We need a radical reorganization of the way in which health care is delivered, and radical changes in financing are required to make that happen. Nobody is even willing to touch that right now, because the power of vested interests -- drug and device manufacturers, medical specialists, insurance companies, big institutional providers -- especially the for-profit hospitals and nursing homes but non-profit academic medical centers as well -- are not going to allow it. They own enough politicians and they are ruthless enough to promulgate sufficiently outrageous lies that we can't even have the discussion we need to be having.
I'm off to Connecticut now, so I'll just leave it at that and say more about it later. But the bottom line is, we have to stop health care from eating the economy. We need to take commerce and greed out of it, and create a new, cost-effective, just and humane, and oh yeah, much cheaper and humbler way of doing this.
And oh yeah. We need universal, comprehensive, single payer national health care. Nothing less.
Friday, October 30, 2009
Yes, I have been reticent
Thursday, October 29, 2009
The thing speaks for itself . . .
Picked this up from Balloon Juice, it must be shouted far and wide:
Evan Bayh, the junior senator from Indiana, is in the middle of a heated debate in the Senate on whether a public option should be included as part of President Obama's health care reforms. An organizer of a group of so-called Senate Blue Dog Democrats, to date, Bayh's been a staunch opponent of any changes to the status quo in this debate. He's worried aloud that any public option would be a nod to socialism and counter to his principles as a fiscal conservative. . . .
His wife, Susan Bayh, sits on the board of WellPoint(WLP Quote) in her hometown of Indianapolis. Over the last six years, Susan Bayh has received at least $2 million in compensation from WellPoint alone for serving on its board.
Now that's fiscally conservative.
There are pills that make you large . . .
but the pills the FDA approves don't do anything at all. Schwartz and Woloshin have a kvetch, that a lot of information the FDA has about the drugs it approves don't make it onto the "label" -- actually a many-page document which is supposed to discuss the risks, benefits, indications and counterindications. The drug companies write these labels themselves, and the FDA just approves them. So, no big surprise, they tend to overstate the benefits and underplay the downside.
However, I take a further lesson from the cases they discuss, which is that some of these drugs never should have been approved in the first place, because they don't actually work. And not surprisingly, these drugs that don't actually work are often among the most heavily marketed and the biggest sellers.
Take Lunesta. If you own a television, you have been exposed to countless visions of formerly sleepless, cranky people passing instantly into sweet oblivion and awaking as though dipped in the fountain of youth. But as it turns out:
Lunesta sales reached almost $800 million last year. Clinicians who are interested in the drug's efficacy cannot find efficacy information in the label: it states only that Lunesta is superior to placebo . . . The FDA's medical review provides efficacy data, albeit not until page 306 of the 403-page document. In the longest, largest phase 3 trial, patients in the Lunesta group reported falling asleep an average of 15 minutes faster and sleeping an average of 37 minutes longer than those in the placebo group. However, on average, Lunesta patients still met criteria for insomnia and reported no clinically meaningful improvement in next-day alertness or functioning.
Oh. So what are we spending the $800 million for?
Well, it's not the FDA's job to decide whether a drug is actually worth anything. It just has to be superior to placebo, not necessarily in any clinically significant way. And while risk of serious adverse effects could make a drug non-approvable in principle, there aren't any clear criteria for deciding when risks outweigh benefits to the extent that a drug should not be approved. Indeed, risks often emerge after approval but seldom lead to withdrawal.
But it has to be somebody's job to make the judgment that it just doesn't make sense to prescribe this drug. That's the agency we don't have here in the U.S. - and no, it's not in any of the Senate bills.
Wednesday, October 28, 2009
About the massive killer flu pandemic
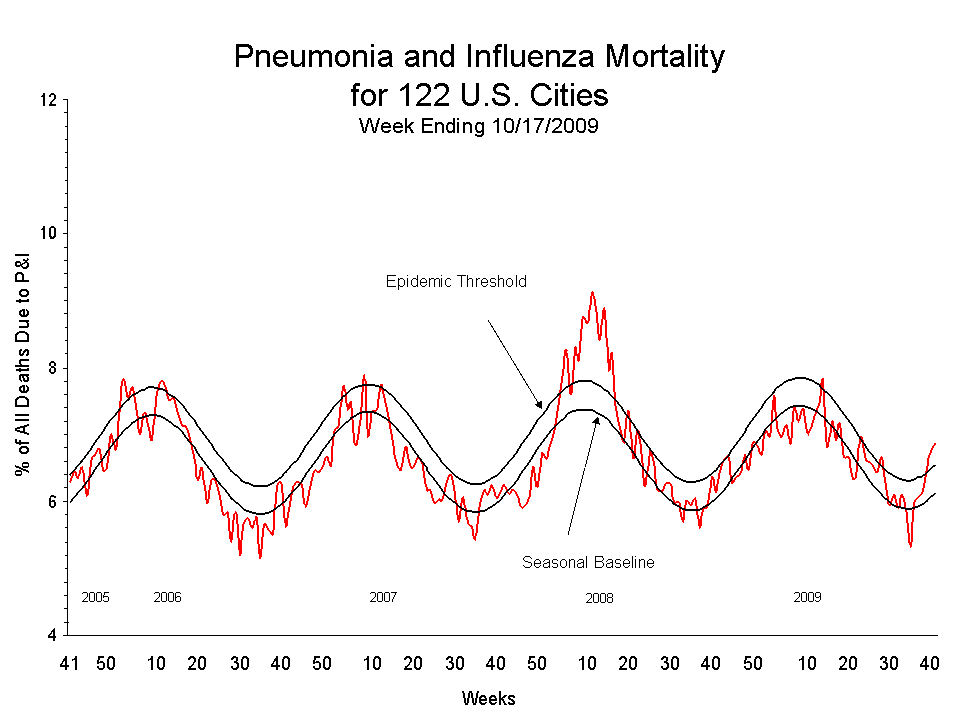
When I made this small enough to fit on the blog it got hard to read. (Click it for a larger view.) Each wave is one year -- the little spike above normal was in 2008. This year, nothing unusual is happening.
Res ipsa loquitur.
This must stop
It's been a while since I've ranted about the pandemic of antipsychotic poisoning in children, but Christoph Correll and colleagues have just reloaded my cartridge belt. Previous studies of the adverse effects of antipsychotic "medications" in children have been flawed because most of the kids had previous exposure to these toxins and were already damaged. That made the new damage seem less.
Correll et al find that when kids are first given these poisonous substances -- aripiprazole, olanzapine, quetiapine, or risperidone -- they very quickly gain weight. A lot of weight, up to 20 pounds in less than three months in the case of olanzapine; and they develop lipid and metabolic abnormalities putting them at risk for diabetes and heart disease. Less than a third of the kids who were prescribed these "drugs," by the way, were diagnosed with schizophrenia; almost half had "mood spectrum" disorders, and a fifth had behaviors that adults didn't like.
The truth is that children are normally emotionally labile and it is not established in any way that there is any such thing as "bipolar" disorder in children; nor that the appropriate response to children whose mood swings or behavior is problematic for adults is to drug them. Most children with emotional and behavioral problems have been victims of some sort of trauma and that's what needs to be addressed, by getting them into a safe environment and providing them with trauma focused counseling which has been proven to work.
But more and more, we're just drugging them. In an accompanying editorial, Varley and McLellan note that in 2003-4, 1% of all pediatric outpatient visits resulted in the prescribing of an antipsychotic. This is a crime on a massive scale. The drug companies got these substances approved for use in adults, but most prescribing in children is still off-label. Nevertheless insidious marketing, much of it the work of physicians who take big payoffs from the companies, such as the distinctly odious Joseph Biederman of the World's Greatest University has produced this epidemic of poisoning.
What's motivating . . .
about listening to a war criminal talk about picking up dog poop? Only in America could a guy who ought to be in a prison cell in the Netherlands end up telling lame stories for 19 bucks a head. What a country!
However, George W. Bush is not the most loathsome politician in the United States. That distinction, without question, goes to His Holiness Joe Lieberman, of the Joe Lieberman Party, representing Aetna Insurance in the United States Senate. On behalf of his sole constituent, Holy Joe promises to join Republicans in a filibuster to prevent the majority of Senators from carrying out the wishes of the large majority of voters, because democracy is bad for Aetna.
Holy Joe says "We're trying to do too much at once. To put this government-created insurance company on top of everything else is just asking for trouble for the taxpayers, for the premium payers and for the national debt. I don’t think we need it now," and "even with an opt-out because it still creates a whole new government entitlement program for which taxpayers will be on the line."
I'm trying to remember the last time Holy Joe moved his lips without lying, but I'm not coming up with anything. All of the above is, of course, a lie. The government sponsored plan in the legislation is financed entirely by premiums, not taxes. It is not an entitlement, it's an insurance plan that people can buy. It does not add to the national debt, it reduces it, because it will be cheaper than what Aetna has to offer, and therefore will require less in the way of subsidies from the treasury for low-income people to buy it.
But Holy Joe knows he can lie all he wants to, however outrageously he wants to, and the corporate media will just reproduce what he says without bothering to point out that it is not true. As in the provided link.
It is, of course, his deep piety and love of G_d that gives him the moral authority to spew lies in the service of his corporate masters against justice and freedom. He's such a good and holy man.
Tuesday, October 27, 2009
Business News
A commenter asks who does own these Blue Cross/Blue Shield insurance companies? Originally, they were all non-profit, but a movement began in the '90s to convert them to for-profit corporations. As Jamie Robinson recounts here, being not-for-profit did not necessarily mean that they operated principally in the public interest. Cozy relationships with hospitals and specialists, limited or no competition, and indulgent regulation all meant that they weren't necessarily working for you.
However, for-profit insurers have investors who inevitably are going to come first, so it's not even an issue. The largest insurer in the U.S., WellPoint, owns the Blue Cross/Blue Shield brand in Colorado, Connecticut, Georgia, Indiana, Kentucky, Maine, Missouri, Nevada, New Hampshire, Ohio, Virginia, Wisconsin, George, New York and California. It is a public corporation. You can buy stock -- it's going for about $45 a share right now, and the share price is prominently displayed at the top of their web site, next to a tab leading to investor info. Some other states' plans are private corporations, but I don't have easy access to a list of which are private for-profit and which remain non-profit.
There were a lot of issues in these conversions about what should happen to the "social assets" embodied in the not-for-profit corporation. In California the conversion was accompanied by a big contribution -- about $6 billion IIRC -- to a foundation called the California Endowment which basically funds projects aimed at health equity. That sounds good, but $6 billion doesn't go far at all in California; as is obvious right now, the good offices of the California Endowment are a fart in a whirlwind compared to the unmet health care needs of Californians.
The main issue, as far as I'm concerned, is that this created a powerful vested interest, with very deep pockets to spend on lobbying and lying to the public in advertisements, which is standing in the way of reform in a way that non-profit corporations would have been much less motivated to do. That was the biggest mistake.
Monday, October 26, 2009
I got nothin',
basically, so go check out TPM's report on BC/BS of North Carolina pressuring Sen. Kay Hagan to vote against any "public option." Their rationale?
Public option?
Government Cooperatives?
Community plan?
Single payer?
No matter what you call it, if the federal government intervenes in the private health insurance market, it's a slippery slope to a single payer system.
Who wants that?
No comment necessary. What I do want to comment on, however, is the nature of Blue Cross/Blue Shield of North Carolina, and most of the other BC/BSs. If you got to their web site and read their annual report and all that you will see all sorts of frou frah about public service and making the world a better place for humanity and saving baby kittens, but in fact, Blue Cross/Blue Shield of North Carolina is a for-profit corporation that, despite posturing as Mother Teresa, exists to make money for its owners -- who, by the way, are conspicuously unmentioned anywhere in the web site or annual report.
Just so you know.
Friday, October 23, 2009
Oh yeah . . .
After a fairly miserable week, I finally feel like myself again -- and that actually feels better than feeling like myself. I think we really need to get sick once in a while to appreciate feeling well. Conversely, I'm more and more sold on Ivan Illich's idea of social iatrogenesis -- that as a culture, we've come to believe that perfect health and freedom from pain is some sort of a human right, and we're just going to keep going to doctors and guzzling pills and having ourselves sliced and diced until everything is perfect. That's one reason for all this influenza hoopla -- the idea that you might feel like shit for a few days is a major emergency.
Listen up buster. Life is tough. You're gonna get sick sometimes. Sometimes it's gonna hurt. Get over it.
Having gotten that off of my thorax, a couple of news flashes, one of them pretty disturbing. From Felix Salmon: "The length of time the average unemployed person has been without a job has been hitting new record highs for a while; it’s now managed to pass the 6-month mark. That’s much higher than any previous peak in this data series." And those folks are exhausting their unemployment benefits -- 7,000 a day hitting the end of the benefit period and now having zero income, last I heard. These people are almost all going to be wiped out -- they'll lose every material thing they've gained in their lifetimes -- financial assets, houses, furniture, cars. They're destitute. And their chances of ever getting it back are very small.
Now that really is pain worth worrying about, and if it continues and doesn't get a whole lot better pretty soon, it's going to put major strain on the social fabric. And it will be all over for the Obama presidency. We've read about people living in tent cities here and there, but the only reason we haven't had Hooverville scale phenomena is because of unemployment insurance, which didn't exist in the 1930s. But it might just be a delayed reaction. Watch out.
Now for something completely different, some investigators are saying that rats become addicted to junk food in pretty much the same way they do to heroin and cocaine. This hasn't been peer reviewed and what is more, people aren't rats (with some exceptions). Still, there may be something to it. Eating habits for many people do seem almost impossible to change. We'll keep watching.
Thursday, October 22, 2009
The world turned upside down
Since people who are chronically ill presumably need health care even more than people who are not, one might hope that people who are not insured are disproportionately those who are young and healthy and just figure they don't need it. And indeed, that's what a lot of defenders of the status quo will say. Alas, it is not so.
As Pizer et al report, low income people with chronic health problems and disabilities have high rates of not being insured, even though one of the purposes of Medicaid is to provide access for that population. Indeed, they have considerably higher rates than the average among all Americans. This is yet another malignantly ridiculous situation in which common sense understanding of reality collides with policy to produce a massive explosion of inhumane idiocy.
The data for this analysis, from the Medical Expenditure Panel Survey, already moves us a step or two away from reality. MEPS asks about nine chronic conditions, but not, for example, cancer or chronic kidney disease, HIV, and others one might think are important. And it's definition of disability depends on functional categories, whereas the relevant category for policy is ability to work, since that's what determines Medicaid eligibility. Many people with disabilities, or course, do work, although bizarrely, many cannot only because they would lose their Medicaid if they took a job. (No joke.)
So already we're a bit askew. Nevertheless the results are instructive. Overall, the MIPS from 2000-2005 has 16.4% of adults under 65 uninsured. (It's more now, of course.) among moderate and higher income people, people with disabilities and chronic health conditions were somewhat less likely to be uninsured than those without; but among low income people, that is not the case. The disparity is most striking in the South, where more than half of people with incomes below 125% of poverty were uninsured, including 32.3% of people with chronic health conditions and 21.5% of people with disabilities.
Yup, the South rises again. The region where political resistance to health care reform is the strongest is the region where 1/3 of low income people with chronic health problems didn't have health care five years ago, and more don't have it today. And what happens when your diabetes is uncontrolled? Oh, not much. You might lose your legs, you might go blind, you might have kidney failure, you might drop dead. But the alternative would be socialism.
Wednesday, October 21, 2009
Remember, you read it here first
The American Cancer Society finally admits that they have been overhyping the benefits and underplaying the adverse effects of breast and prostate cancer screening.
"We don’t want people to panic,” said Dr. Otis Brawley, chief medical officer of the cancer society. “But I’m admitting that American medicine has overpromised when it comes to screening. The advantages to screening have been exaggerated.”
Abstract of the JAMA article is here. Since you are too low-borne and no account to read it, I will summarize for you. When you start widespread screening, you will, obviously, have a sudden jump in the incidence rate of cancer, because you're detecting more of it. What you want to happen is that after time, the incidence of serious disease and death goes down, because early detection has prevented many cancers from becoming serious.
What has actually happened is that the incidence of prostate and breast cancer have doubled; but the incidence of serious disease and death has declined little for both types of cancers, perhaps not at all due to screening. Periodic screening may be good at detecting early stage lesions that will never develop into meaningful disease before the person dies of something else; but tend not to find more dangerous cancers early enough to make much of a difference. And that appears to be what is happening. A large burden of morbidity and treatment for innocuous lesions that would never have caused a problem, in exchange for a very small reduction in the rate of serious disease and death, if any.
Mass screening would be much more useful if we could distinguish the dangerous lesions from ones that just bear watching, but as of now, we really can't. The shameful truth is, however, that without having good evidence that screening really does save lives or that the benefits outweigh the costs, the ACS and disease-specific organizations have undertaken mass campaigns over decades to try to get everyone to be screened. Of course there is money to be made at every stage, from radiography to lab to surgery and chemotherapy. Is that why they jumped the gun on the evidence? Who would think such a thing.
And while we're on the subject of what you read here first:
As I and others have been saying for some time now, the influenza surveillance data which has been used to describe the novel H1N1 pandemic is based, not on actual confirmed cases, but merely on the number of people who present with flu-like illnesses. For some reason, the public has been told to assume that most of these are in fact cases of novel H1N1 influenza, but that has not been established. CBS News now reports that the overwhelming majority of people who have been tested did not have novel H1N1 influenza, or even, in most cases, have any form of flu. Hmm.
Update: Kathy's comment reminds me that I should clarify something. The new position from the American Cancer Society refers only to mass screening of the general population. If you are at high risk -- for example, because you have a "first order relative" (parent or sibling) who has had breast cancer, especially at a relatively early age, your cost/benefit profile is very different, and mammography makes much more sense for you. I'm not here to give individual medical advice, but to talk about broad policy. You should make your own informed decisions, hopefully in consultation with your physician.
Tuesday, October 20, 2009
Safety, cost, and justice
A commenter suggests that we will not have a safer food supply unless we are willing to accept higher food prices. I'm not sure this follows. Obviously some money would have to be spent to improve food safety, by somebody, but the policy equation is not safer food = more expensive food.
I don't know that anyone has tried to calculate how much, if anything, it adds to the cost of specific foods to handle them safely, but it can't be very much. After all, the vast majority of growers, processors, distributors and retailers manage to sell food at competitive prices without poisoning anybody. Conversely, if you do poison people and get caught, it could cost you a whole lot in lawsuits, enforced shutdowns, even permanent extinction as a business. Any food-related business has to invest in safe handling, the issue is really whether they exercise diligence, which is probably not very much related to spending money.
Such relevant expertise as I have comes from health care safety improvement, but I expect it's applicable. The Institute of Medicine famously issued a report in 1999 entitled To Err is Human, which reviewed the nature and extent of medical errors and solutions. Their central conclusion can be found in this paragraph:
Health care organizations must develop a “culture of safety” such that their workforce and processes are focused on improving the reliability and safety of care for patients. Safety should be an explicit organizational goal that is demonstrated by strong leadership on the part of clinicians, executives, and governing bodies. This will mean incorporating a variety of well-understood safety principles, such as designing jobs and working conditions for safety; standardizing and simplifying equipment, supplies, and processes; and enabling care providers to avoid reliance on memory. Systems for continuously monitoring patient safety also must be created and adequately funded.
While it does assert that systems must be funded, that does not necessarily imply an increase in the net cost of providing health care. Standardizing and simplifying, and avoiding reliance on memory, can save money. Health care organizations increasingly are being brought under outside scrutiny to assure patient safety, by funders, state departments of health, and accrediting organizations. But nobody complains about the cost or claims that this adds to the cost of health care. Presumably it reduces it in the long run, since it costs an awful lot when you amputate the wrong leg or give somebody a drug overdose.
I expect the same is true for the food industry. What is needed is accountability, and that may require some public spending -- i.e., taxpayers' money -- to pay for more extensive and effective inspections. But it will be a very small amount in the overall picture of government spending. I think most people will think it is well worth it.
Finally, although libertarians have a reflexive aversion to intrusive government, the truth is that assuring food safety will increase our individual liberty, not constrain it. I want to be free to buy food where and when I will with confidence that it won't make me sick or kill me. Depriving me of that confidence and opportunity makes me less free. Is it worth a few cents in taxes? You betcha.
Update: I should have mentioned that there is no consensus that we've necessarily gotten much closer to a really safe health care system. And insufficient external accountability is generally thought of as the main reason. The linked blogger has a fair and balanced view, so you decide.
Monday, October 19, 2009
Health diary
The late Irving Kenneth Zola was going to chair my dissertation committee, but he died the day I learned I had received funding for the study. Irv, among other physical problems, was diabetic, and as can happen with diabetes he had a heart attack and was not aware of it due to neuropathy.
Anyway, in his seminar Problems and Issues in the Sociology of Health and Illness, he asked us to keep personal health diaries -- write down every day whatever we could about our state of health and experience of health and illness, however defined. I certainly don't want to inflict such a narcissistic project on the world, but I think my recent - nay, still current - bout with a food-borne illness is mildly instructive. I was out in the country finishing up work on my rustic cabin and as I often do I bought lunch at the local general store. They offer an unappealing assortment of bland deli salads but they are also the only place in town, and I mean that: there is exactly one store of any description.
Well, it hit me at about 12:30 a.m. on Sunday. I got no sleep that night. I was in and out of the bathroom every 10 minutes, and it lasted all the next day. Since it was a Sunday I wasn't missing out on a whole lot of productivity by lying on the sofa between excursions to the water closet and watching steroid abusers in plastic armor beating the shit out of each other. However, I'm still pretty groggy today and I have continuing abdominal pain. If the timing had been different I would have missed a day or two of work -- not a huge deal maybe but the economic costs add up, or at least they would if I did anything of economic value.
CDC estimates that 76 million Americans get sick from food-borne illnesses every year, that's about one quarter of us all, so we've all been there. It's mostly just an extremely unpleasant experience and a sick day, but there are 300,000 hospitalizations and 5,000 deaths, so on the whole it's well worth making a significant investment to avoid it.
And here, once again, is a compelling example of why "free markets" are a hallucination. As a consumer, you have absolutely no way of knowing whether the food you buy is going to make you sick. The contamination is invisible and you can't observe how it is handled at any stage from farm to factory to grocery or restaurant. In some cases you might be able to make a pretty good guess about what meal it was that made you sick, but that doesn't empower you as a consumer either. I don't know whether the problem was with the way the salad was handled at the General Store, or their immediate supplier, or someplace way up the manufacturing chain, e.g. the mayonnaise factory. So boycotting the store isn't going to do me any good.
The only entity that can protect us is Big Government -- the nanny state. I suspect that there is no Board of Health of any kind to inspect the General Store, but we generally depend on local governments to inspect grocery stores and restaurants. Good luck with that. The Dept. of Agriculture's Food Safety and Inspection Service is responsible for producers of meat, poultry and eggs, and the FDA is basically responsible for everything else. However, the FDA contracts half of the work out to the states, and it doesn't do nearly enough to assure that the states are doing the job -- which to a substantial extent they are not. As for imported food, fuggedaboudit. "Just 1.3% of imported fish, vegetables, fruit and other foods are inspected — yet those government inspections regularly reveal food unfit for human consumption."
As I sit here with my abdomen cramping, I am displeased. Of course, it's not influenza so it doesn't matter.
Friday, October 16, 2009
Civil War
The Commonwealth Fund recently came out with its annual state scorecard on health system performance. You may be interested in seeing how your own state is doing. It is instructive, first of all, that since we do not have any effective national policy to shape health care system performance, the variation among the states is enormous. You will not see this in civilized countries that have coherent national health care systems.
But I particularly want to draw your attention to Exhibit One, (click to enlarge) which shows an overall ranking of the states. Notice any patterns there? What do you think would happen if we colored those states red and blue depending on the likelihood that their senators will vote for national health care reform? Of the bottom ten, only Illinois gets a gold star. Of the top ten, South Dakota and Nebraska get a split, although we'll have to see what Ben Nelson ends up doing; Joe Lieberman might be a no vote but he doesn't represent his state; and Maine is likely a no although Sen. Snowe is still teasing us. Otherwise, they're all on board.
The picture is more mixed in the middle, and this picture interacts with population density, regional culture and other factors that influence both politics and health system quality. Still, the states with the worst health care systems are the least likely to have elected representatives who support change, while the states with the best systems are mostly for it. Why do you think that is?
{kind=link}
Thursday, October 15, 2009
The ongoing holocaust
I'm fired up, and I'm also pretty well pissed off. Spending the day at the New England Regional Minority Health Conference just stirs up all that bile about the grossly misplaced priorities of the corporate media. Here's one very simple way of getting across a big idea. Former Surgeon General David Satcher and colleagues back in 2005 used vital statistics to figure out how many excess deaths would be prevented every year in the United States if the mortality gap between white and black people were closed.
The answer is 83,570. As one of the co-authors, Adewale Troutman told us yesterday, that is equivalent to loading up a jumbo jet and crashing it into the ground with no survivors every single day, not for a week, not for a month, not for a year, but year after year, apparently forever, since this gap is not getting any narrower.
But you probably didn't know that because the only public health issue in the world is influenza.
It is not only African Americans who die prematurely, of course. Poor health and premature death are the likely fate of everyone who is socially disadvantaged. Poverty, poor nutrition, an unhealthy physical and social environment, inadequate education and lack of opportunity for fulfilling work, social subordination and lack of control over one's circumstances, discrimination -- these are the sources of health disparities. Health equity is the civil rights movement of our time, because it encompasses every element of a just society. Health equity has little to do with medicine. It has to do with agricultural policy, land use policy, transportation policy, educational policy, economic policy -- public health is about everything.
It's much easier to talk about influenza because it has nothing to do with difficult questions of justice and equity. Rich white people are interested in it because it affects them, just the same as everyone else. It's not a threatening subject at all. It has no political content. As far as I know, Rush Limbaugh and Rachel Maddow have exactly the same opinions about it. So that's why we hear so much about it.
Wednesday, October 14, 2009
Road trip
I'll be at the New England Regional Minority Health Conference in Providence today. I don't know whether I will be connected to the Great Web of Being. If so, I may give you my usual thrilling conference live blogging. If not, today's post will be late. Que será, será.
Tuesday, October 13, 2009
A medical mystery
Specifically, why is there a persistent movement to deny the safety and efficacy of vaccination? I can understand why there are creationists -- religious beliefs are deeply embedded in the culture, the priesthood has a strong vested interest in its own power and great sway over its followers, and people feel threatened by challenges to cherished and comforting beliefs.
I understand that racism fuels the birthers. AIDS denialism has multiple psychological underpinnings, but they are all related in one way or another to the stigma associated with the disease. Like the modern antivaccination movement, it got a big boost from a rogue scientist -- leading virologist Peter Duesberg who became a major crank. I believe what happened to Duesberg is that he started out asking legitimate questions and wanting more proof, but then found himself too deeply dug in to bow out gracefully when the questions were answered and the proof came. This is classically how rational people evolve into cranks.
Andrew Wakefield, who started the vaccine scare, may be a different story -- he appears to have faked his data for the simplest of all reasons, money. And now of course he cannot admit that. But granted the scare began initially because of a scientific publication, why won't it go away now that Wakefield has been irrefutably debunked? Yes, we had dishonest self-promoters such as Robert Kennedy Jr. link to the anti-vaccination movement as a phony liberal cause in order to build his own fame, probably in hopes of running for office as a crusader against the medical-industrial conspiracy. And we have the celebrity (why?) Jenny McCarthy using her public soap box to keep it going.
But still, there have to be deeper reasons why people so badly want to believe in this. You can't just stand up and start spouting any old nonsense and expect it to gain traction. Now that we have all this publicity about influenza people like Bill Maher and various pseudo-scientists on the Huffington Post are coming out of the woodwork to tell people not to get the vaccination for novel H1N1 influenza.
Now listen up folks. That's just plain nuts. I am notorious for believing that the corporate media and Daily Kos talk about the flu too damn much and don't talk nearly enough about other public health issues that are more important because they a) affect more people, b) cause much bigger problems because when they don't kill you outright, unlike the flu they don't go away in a few days but can cause long-term sickness and disability, c) are always around, not just in a brief episode and d) have political content and dimensions of justice.
But: You don't want to get the flu, H1N1 or any other kind. It will make you feel like shit, be out of commission for a while, and yes, might just turn into a serious disease or even kill you even though that's unlikely. And you might transmit it to others, so it's not just your own choice that's involved. Flu vaccines, novel H1N1 or otherwise, have a long record of being very safe and very effective. About the worst thing that can happen to you is a mildly sore arm. Advising people not to do it is not just mistaken and unhelpful, it is evil.
When you get the chance, get the shots. You'll need two this year, one for the so-called "seasonal" flu and a separate one for the novel H1N1. Get them both. End of story.
Monday, October 12, 2009
A world historic figure
Columbus Day undoubtedly celebrates a significant event in world history. If Columbus hadn't made his famous voyage, it would have taken the Europeans at least a few more years to find out that the lands to the north and west of which they were vaguely aware were far more extensive than they had realized. The result would have been to delay the dispossession and holocaust of the people's of the Americas, the mass enslavement of Africans, the destruction of the North American forest and prairie, the extinction of the passenger pigeon, and Jon and Kate, by a decade or two.
We are taught in school that Columbus was a genius who figured out that the earth was round, while everybody else thought it was flat and he was going to sail off the edge, so they all laughed at him. Actually that's not why they laughed at him. Sailors knew perfectly well that the earth was a sphere -- the ancient Greeks had figured that out and they had also calculated its size, quite accurately. Columbus's bright idea was that the earth was only 15,000 miles in circumference, and that's why people laughed at him, quite rightly. If he hadn't blundered into the Antilles, Columbus and all his crew would have perished because they were not provisioned for a journey of 17,000 miles. In fact they barely made it to San Salvador. So Columbus may have been a heroic entrepreneur, but he was also an utter fool, just an inordinately lucky utter fool.
The Spanish, on the other hand, turned out to be unlucky fools. Those Indians or whatever they were had gold. The Spanish thought they had struck it rich, as they hauled caravel after caravel laden with plunder back to the homeland. The result was not that they became wealthy. All they had, after all, was big piles of useless shiny metal that happened to be what they were using for money at the time. Money is only worth what you can buy with it and if you have more money and the same amount of stuff, you have not wealth, but inflation -- in this case a ruinous inflation that left Spain the most impoverished and undeveloped nation in Western Europe right up until the end of the 20th Century.
Columbus Day in the U.S. is celebrated mostly as an Italian-American festival, on the grounds that Columbus was born in Italy. An odd conceit, as Italy had nothing to do with his voyages, no interests in the Americas, and Italians didn't even start coming here in substantial numbers until 400 years after the famous voyage, plenty of time for some other European to have blundered onto New Haven.
But, it's a day off from the salt mines, so I'll make the most of it.
Friday, October 09, 2009
Credit where it's due
I have tossed my share of snark in the direction of National Public Radio, but this time, they get their full complement of "l"s. I thought this story by Alix Spiegel was exemplary journalism. This is what the profession ought to be about, and is so seldom.
It's also a great follow-up on yesterday's post and gives me a chance to make an additional important point. You'll notice the URL for this site - health vs medicine. That represents a basic premise that I probably don't bring to the foreground often enough. Obviously medicine is supposed to be making us healthier, but it's just as much the enemy of good health as it is the champion. This happens in multiple ways. Taxonomies are always a little bit arbitrary -- you can lump or split as you like, and organize groups of phenomena in various ways. I'll just make a crude first effort here.
First, as Spiegel's story makes clear, doctors may simply do things that hurt more than they help. They have enormous power over our bodies, including the power to cut out essential parts. We don't generally know any better than to trust their judgment, but it isn't necessarily very good. This is partly due to the general culture and the specific medical culture that's both embedded in it and highly influential. We have a bias toward action, toward doing something; we're all about being bold and decisive and heroic. And we have a lot of faith in technology and anything that wears the guise of science. But the shocking truth is, much of medical intervention is not based in science at all, is not driven by evidence, but by physician's intuitions and customary ways of doing things. And, let's bite the bullet and make this painful admission: doctors are paid to do stuff, and the more radical their actions, the more they are paid.
Second, by holding out the false promise of perfect health and great longevity, medicine distorts the culture and our individual response to pain and disability. Ivan Illich, who was a Catholic priest and had that Catholic fatalism, was an aggressive proponent of this view. It showed up in Keith Olbermann's special comment, where he seemed to champion the defeat of death and worship at the altar of medical miracles. Life sometimes throws adversity our way. Not that it isn't worth trying to cure disease and relieve pain and give people a good lifespan, but we also just have to suck it up and deal with it sometimes.
Third, our excessive faith in medicine diverts our attention from the very important social determinants of health, to which Bix eloquently alludes in a comment on yesterday's post. Social justice begins long before we even think about universal health care. Sure, if we had it our society would be more just than it is now but we would still have huge inequalities in health and life expectancy because of all the other inequalities that would remain, for which medicine does not have the answer.
And fourth, every dollar we spend on medicine is a dollar we don't spend on something else, whether it's a modicum of justice, or a measure to promote the general welfare such as generating cleaner energy or providing parks or mass transit or clean water.
That's why health care reform is only the beginning. And the wrong kind of reform, that just extends the present medical pathology to everyone, and sucks more money and more social and cultural capital out of us all, will be worse than nothing.
Thursday, October 08, 2009
Half right is still wrong
I don't know how many of you managed to keep your eyeballs deglazed long enough for all of Olbermann's "special comment" last night -- the best I could do was check in from time to time between innings. But I got the gist. Keith thinks the way most people do about health and health care. He think they are synonymous, and he thinks that justice and compassion demand that we do everything possible, every time, for everybody, even if it means just giving them one more day of life because life is infinitely precious.
That is indeed the basis on which many people rest their demand for universal health care insurance, but as I have pointed out here many times, if we really believed that, there would be no way to provide universal health care. It's totally paradoxical. I've discussed this many times, you can go here if you want a refresher. But the discussion on yesterday's post got me to thinking that one important way in which our cultural biases are clearly manifested is on death certificates. Yes, I've also gone there before, but it's worth revisiting in this context.
The so-called Leading Causes of Death are familiar. In the U.S. they are, in order with the number of deaths attributed to the cause in 2006:
Diseases of heart -- 631,636
Malignant neoplasms -- 559,888
Cerebrovascular diseases -- 137,119
Chronic lower respiratory diseases -- 124,583
Accidents (unintentional injuries) -- 121,599
Diabetes mellitus -- 72,449
Alzheimer’s disease -- 72,432
Influenza and pneumonia -- 56,326
Nephritis, nephrotic syndrome and nephrosis -- 45,344
Septicemia -- 34,234
Intentional self-harm (suicide) -- 33,300
Chronic liver disease and cirrhosis -- 27,555
Essential hypertension and hypertensive renal disease -- 23,855
Parkinson’s disease -- 19,566
Assault (homicide)-- 18,573
All other causes (residual) -- 447,805
Now, there is a lot wrong with this picture. All but three of the listed causes are disease labels, and Keith rightly thinks that heroic doctors can do something to keep people who have these diseases alive longer, even if they can't cure them. Even in the case of the "non-disease" causes, if you will -- unintentional injury, suicide and homicide -- some people who suffer violent trauma can be saved.
But let's step back for a moment. What is the point of generating this list? What guidance does it offer for policy, or for institutional or individual action? The answer is almost none that I can see.
In the first place, since none of us can possibly avoid death, the best we can do is choose among causes. If one doesn't get us, another will, so if we reduce or eliminate any of these causes, it will just cause another to increase. It's a zero sum game. What we really need to be asking is not whether people die of heart disease or pneumonia or cancer. The only sensible questions are what people's dying is like for them and those around them, how well they lived before that, and whether they had enough time to do what they wanted to do, given that they aren't going to have forever. If you live to be 85, in excellent health, productive and fulfilled the whole while, and on your 100th birthday drop dead of a heart attack, your death certificate will say "diseases of the heart." It will not be a tragedy.
On the other hand, if you spend the years from age 50 to age 100 in chronic pain, demented, and socially isolated in a nursing home, and then your death certificate ends up saying "influenza," it will be a tragedy alright, but the tragedy will not be your death and influenza will not be the enemy.
In the second place, are these "causes" of death at all? Why do people have heart disease? Why do people have lower respiratory disease, or cancer, or diabetes? (Diabetes is actually two completely different diseases that have nothing to do with each other except for some overlap in the treatment, which makes the list all the more absurd.) Why do people kill themselves, or each other? Once we start asking these questions, health care stops looking very important after all. People are killed by tobacco, bad nutrition, alcoholism, sadness and anger, poverty -- and these causes of death tend to go along with happening too early, being ugly and painful and sad, and being just the final paragraph in a long story of disease or pain or despair.
And if we spend all our money on doctors and high tech scanners and proton beams and gamma knives and organ transplants, we won't be able to do anything about any of that stuff. In fact, we'll just make it worse.
Wednesday, October 07, 2009
The Real Cost of Irrational Flu Obsession
I have said more than once that the influenza "pandemic"* is the Shark Attack or Missing White Woman story of public health. Yeah, it is actually happening, but it isn't nearly as important and the stuff we don't talk about because we're talking about flu all the time. One example is pneumonia -- the vast majority of the time, not associated with influenza -- which kills a little kid once every 15 seconds.
Really. Two gone while you have been reading this. The organisms most commonly responsible are not influenza virus, but Haemophilus influenzae type B (Hib) and pneumococcus, and there are others. Of course you didn't know that because you were busy reading about influenza.
A broad coalition wants to break through to your consciousness with World Pneumonia Day. It's a little hard from the web site to figure out that the date is November 2, but apart from that odd glitch, there's lots of information there, so check it out.
Of course, kids rarely die of these diseases in rich countries, because they are better fed and better housed, and so stronger and less susceptible; they are more likely to be vaccinated against many of the responsible organisms; and they get medical care if they need it. So this is very much about the social determinants of health, not just those nasty little microbes. In other words, this is about social justice and politics. Which is probably why we hear so little about it. Influenza is much safer to write about, because it is politics-free.
*By the definition they had to re-write in order to turn novel H1N1 into a pandemic, we have a global influenza pandemic every single year.
Tuesday, October 06, 2009
The Nobel Prize in Physiology or Medicine . . .
and why I have somewhat mixed feelings about it. For those of you who don't already know, the prize this year was awarded to researchers who have elucidated the functioning of structures on chromosomes called telomeres. As a crude analogy, they are like those little plastic doodads on the ends of your shoelaces that keep them from unraveling. (I believe I once read somewhere that there is actually a name for them; if anybody knows it, let me know.)
Anyway, whenever your cells reproduce the telomeres have to be rebuilt on the new chromosomes, but there's bad news: they get a little shorter each time and eventually, the chromosomes degrade and the cell line gets old, tired, and useless. This turns out to contribute to the inevitably fatal, incurable disease with which we are all born, which typically gets us sometime after three-score years and ten. So, if we could preserve those telomeres, our shoelaces -- I mean our chromosomes -- would be immortal, and maybe we'd have one more key to curing the disease of aging.
But there's more bad news: evolution gave us this telomere shortening, and there is what appears to be a very good explanation for it. Immortal cell lines are dangerous, because they just might be cancer. Most of our cell lines have to divide only a few times during our reproductive years, so evolution has no reason to preserve those telomeres; indeed, it has a good reason to see them erode, because that is one more hurdle cancer cells have to overcome in order to become malignant. In other words, this component of the aging process protects us against cancer, which otherwise might get us early in life.
So far, our understanding of telomeres has not yielded anything useful, but it might eventually. We might be able to use it to prevent the immortalization of cancer cells, and so cure or prevent cancer; and we might be able to use it to prevent or even reverse elements of the aging process. On the other hand, these two goals might be largely irreconcilable and the knowledge might not turn out to be very useful after all.
But what if all this does lead to more effective cancer treatments, or even the Fountain of Youth? As I wrote earlier about another potential treatment for aging, resveratrol and similar compounds, there could be downsides. But more than that, a vast investment in basic biomedical research -- probably many tens of billions of dollars, at least -- lies ahead in pursuing this particular grail. If it leads anywhere, comparable sums will be spent on turning knowledge into safe and effective treatments, and providing those treatments to those people wealthy enough to afford them, whose benefit will consist of exceeding the natural life span.
Meanwhile, I shouldn't have to tell you but I probably do that today, on planet earth, 20% of all deaths are of children under five years old. Life expectancy at birth right now in Afghanistan is 41 years, and in most of Africa it's under 60 and even under 50 years. We're far from number 1 but we're already up to 78 years. Those tens or hundreds of billions of dollars could wipe out those inequities and save all those kids. Yes they could. But instead we'll invest them in trying to get rich people to live to be 100-120 instead of just 80-100. I dunno about that.
Monday, October 05, 2009
Another installment in our continuing series
entitled "More is Less." I vaguely recall referring some months back to two studies of prostate cancer screening published in NEJM, which you can read here and here due to a special dispensation extended to you ignorant ruffians for this one occasion.
With a little help from Jennifer Stark and friends in the new BMJ (not, alas, similarly available to the rabble), I want to help you understand the bottom lines on these studies, and in particular, how different it all seems depending on how you frame it. In the U.S. study reported by Andriole, et al, the death rate from prostate cancer after 7 to 10 years of follow up in a group assigned to routine screening was actually higher than the death rate for a group assigned to "usual care." Some in the intervention group were not screened every year, and some in the control group were screened, but the former group did have a much higher overall rate of screening. The difference was deemed "not statistically significant," which means it could have been due to chance, but it certainly seems highly unlikely that screening yielded any substantial mortality benefit over this time. Of course the follow up is short.
The European study by Schröder and the gang did find a reduction in death rates over average follow-up of nine years for men who were offered PSA screening of about 20%. That sounds pretty good, huh? But here's the key point I want to shoot you with "like a diamond bullet right between the eyes" -- you would have to screen 1,410 men to avert one death; 76% of positive tests would have been false positives leading to unnecessary anxiety and biopsies; and you would have to have treated 48 cases of actual prostate cancer to avert one death, because a) lots of men with prostate cancer never die from it or even have symptoms and b) some men who are treated die of the disease anyway. Treatment can result in incontinence, erectile dysfunction, and all kinds of pain and expense.
This is the importance of reporting, not relative risk, but absolute risk. Telling someone that you can reduce their chance of dying from prostate cancer by 20% sounds pretty good. But telling them there is a 1 in 1,400 chance that they will benefit; a 12% chance that they will have a false positive test and have to go through all the sequelae; and 3.5 chances out of 100 that they will undergo prostate cancer treatment and not in fact benefit from it, does not sound nearly so good. It will, however, make a whole lot of money for oncologists, surgeons and radiologists, which might just be one reason why they are all in favor of it.
As Doctor Ruth says, I'm not a real doctor, I cannot advise. Talk it over with your real doctor. But do show him or her these true facts.
Saturday, October 03, 2009
I'm baaaacckk
Sorry, didn't have connection to Intertubes at the conference site yesterday and I was too tired when I got home to put anything up. Having recharged the batteries and refreshed the attitude, and being stuck here on a very gloomy, rainy day, I give you a rare Saturday post.
First, Kathy, not to mention the rest of you, may be interested in this health insurance story from hell. The protagonist/victim is a medical resident, no less, and she can't get the insurance company to understand that yes, they are supposed to pay her claim and she does not actually owe $6,000. For years she can't get them to understand that, maybe, just maybe, because they don't want to. My advice, Kathy? I can't remember whether it was Keith Olbermann or Jon Stewart who came up with this originally, but it's good: send the bill to Max Baucus.
Now, as for HIV, the news is pretty much on the same trajectory it's been on since I reported back from Mexico City last summer. Treatments continue to get easier to take and less toxic, but no cure and, sorry, no vaccine is in sight. The trial in Thailand that caused all the flapdoodle and hoohah last week? All the information we have is a press release, which is very bad form to begin with, but from what we can tell, there are some puzzling features of the result. The rate of new infections in the active arm appears to have been somewhat lower, but people who did get infected had the same degree of acute viremia and the same disease progress whether they were vaccinated or not. It's all very technical but what this seems to mean is that if the combination vaccine worked, it worked on a different component of the immune system than hypothesized.
However, we are all still wondering if it really worked at all. The number of infections in both arms was very low, which means that very subtle methodological problems could compromise the finding. The degree of efficacy could well be overestimated just because of chance, and by a lot; even the published estimate is not good enough to make this something that could every be deployed. Any vaccine is still a good ten years away, and unfortunately, ten years has been the Friedman Unit in this field for the past twenty years.
There is work going on on new prevention strategies, such as giving low-dose antiretrovirals to people at high risk, such as sex workers and HIV-negative partners of HIV-positive people. The problem is that these strategies also are less than 100% effective, which means you need to continue to use condoms, but maybe if people think they're protected by the pills they will decide they don't need the condoms after all, plus which they might not always take the pills, not to mention the expense -- you get the idea.
This is all very frustrating. Not that we haven't made some lemonade out of it all. HIV has turned out to be a highly revealing natural experiment which has taught us a great deal about the human immune system, and a great deal about the sociology of health and illness as well. Much of what we have learned has helped us deal with other diseases, and other social problems. On the social front, I would even go so far as to say that the HIV epidemic was in considerable part responsible for stimulating the activism which has led to such dramatic changes in our own country and Europe in attitudes toward the diversity of human sexuality; and the movement (as limited as its success may be so far) to adopt non-punitive, harm reduction approaches to addiction.
In other words, this is a challenge to which many people have risen, although many, sadly, have responded disgracefully, most of them on the political right I might add. But it is a challenge that is still with us and will be for a long time. And oh yeah -- the rate of new infections in the world continues to exceed the rate at which the availability of treatment expand by more than 2 to 1. We're still deep in the woods.
Thursday, October 01, 2009
Where I'm at
I am at the Social and Behavioral Sciences Network Meeting of the Centers for AIDS Research, which are NIH-funded research centers around the country and which, as you may already have guessed, have a social and behavioral sciences network.
David Bangsberg this morning told us something rather interesting. You may remember that many people -- including high officials of the previous administration such as Andrew Natsios -- insisted that there was no sense in providing antiretroviral treatment to people in Africa because they are incapable of following drug regimens. As Natsios memorably said, they don't even have clocks.
As it turns out, the percentage of people in Africa who stick to their HIV drug regimens is a lot higher than the percentage of people here in the U.S. And that's true even though for many of them, it costs 30% of their monthly income just to travel to the clinic every month to pick up their pills, not to mention a whole day away from the fields or whatever their source of sustenance may be.
How do they do it? They draw on social capital -- family members and neighbors give them the money, watch their kids and tend their fields while they are gone. Why? Not only because the people live in close-knit communities, but also becauase, before they got the drugs, they were sick and could not work. Others had to take care of them, while they couldn't pull their own weight economically. Now they are up and around again, working, helping take care of their neighbors' kids, giving back. And so the community depends on them to take the pills, because that's what keeps them a productive, giving part of the whole.
Think how different that is from the context of antiretroviral treatment here in the U.S. And also think about what it tells us about our prejudices and our limited and downright foolish view of the rest of the world.
At a conference today . . .
I don't know whether they will grant me connection to Your Intertubes. If they do, and anything mildly interesting is going on, I'll post something. If I don't, you know why. Or rather, I do have something to say but it might not happen until late today.