The ice isn't melting yet in New England, but maybe the figurative ice is starting to melt in the U.S.A. The schemes of the administration to turn reality into a thought crime are falling apart. It turns out that burning fossil fuels does cause global warming, that mercury is toxic, and that evolution is an established scientific fact, and discussion of these truths is again permitted.
One effort at newthink that got somewhat less attention was the attempt to make racial and ethnic inequality disappear. Political officials at HHS last year attempted to rewrite the annual report on health disparities (produced by the Health Resources and Services Administration under a Congressional mandate), so as to minimize findings of inequality and injustice. They got caught. The attempt in California to pass a ballot initiative forbidding the collection of public health data by race and ethnicity was soundly defeated. The good people of California do not agree with the proposition that what we don't know can't hurt us.
And now we have a new report from the National Committee on Vital and Health Statistics (PDF) calling for more and better data on racial and ethnic disparities in health. One of our biggest problems in this area is the official federal system for classifying the population, which is based on 19th Century concepts of biological race. We get to be White, Black, Asian, Native American, or Pacific Islander, and then we get to choose one "ethnicity": Hispanic or not Hispanic.
That's not how people identify themselves, and it's not who they are, and it's not part of what determines their health status or the quality of the health care they receive. In Massachusetts, for example, 84% of white, non-Hispanic mothers get "adequate" prenatal care (according to a common standard), and 79% of mothers of Cuban ethnicity get adequate care, but only 64% of Puerto Rican mothers do. If you lump all the "Hispanics" together, you won't know this.
Black doesn't mean African American -- people classified as Black might also be Haitian, Jamaican, or Nigerian. Just to show how reflexively people in the U.S. think in terms of race categories, the New York Times once said that every heavyweight champion since Sonny Liston has been African American. They were forced to print a correction noting that Lennox Lewis is a subject of Her Royal Highness, Elizabeth the Second, rather than our own monarch.
In order to understand health disparities, it's also important to know other information such as people's immigration history, preferred language, level of education, etc. We also need more reliable data about ethnicity, based on people's self-identity, not the guess of a hospital clerk, jammed into procrustean categories. NCVHS has now proclaimed this. Whether the administration will do anything about it, or continue to try to back into the future, that's another question.
Tuesday, February 28, 2006
Reality is on the March!
Monday, February 27, 2006
The Romance of the Highway
I've been working with some colleagues on a proposal to study the exposure that people living along major highways experience to hazardous emissions from motor vehicles. The physico-chemistry and biology of this problem are not my department, but I've been getting an education. My mission, which I suppose I have chosen to accept, is to study people's knowledge, attitudes and behaviors about highway air pollution.
What I have learned from my environmental science and physician friends was a bit of an eye opener. Most of what we know about air pollution levels in the real world comes from a small number of monitoring stations, which are used to characterize pollution over wide areas -- no smaller than zip code size. But in fact, the pollution people are exposed to varies enormously over just a few tens of meters near highways. You might think that an urban avenue, with idling diesel buses and cars backed up in traffic is worse, but you'd be wrong. Traffic on the interstate puts out some bad stuff, particularly microscopic particles of soot. The natural defenses in our sinuses and lungs can't filter these out, and they go right into the alveoli and then get into the blood stream.
Believe it or not, while you are probably most worried about air pollution being a risk factor for respiratory diseases and lung cancer, these particles apparently cause inflammatory reactions which increase the risk of heart disease, and exposure to highway pollution has actually been linked directly to increased rates of heart attacks and death. This is not a huge factor -- the stuff you already know about, like smoking and diet and exercise and obesity -- are much more important. Nevertheless it's something that people can't control, except by living somewhere else, which makes it a special kind of concern from an ethical and public policy point of view. And, as you might expect, locations near highways are less desirable so that's where low-cost housing is likely to be and that's where low-income people are likely to live. Again, we're talking very small increments of distance - the pollution falls off rapidly within 100 meters or so.
What I have found out, in what is my department, is that people's perceptions of their risk from air pollution are not related to their actual exposure. People think of air pollution as coming from factories and power plants, but motor vehicles are just as important, in fact much more important, for people who live near highways. The problem is, they don't know it.
Sunday, February 26, 2006
Ricin, Schmicin; or, The Terrorists Have Won
In my self-torturing effort to keep abreast of the zeitgeist, from time to time I look in on the evening network news. Last night NBC and CBS both devoted a few seconds to the world historical disaster in Iraq; and featured long, breathless stories about a University of Texas sophomore who found a mysterious white powder in a roll of quarters. As I presume you know by now if you have poked your head above the blast wall, she called the police who used a field test which yielded a positive result for ricin, whereupon they evacuated the dormitory and men in moon suits started hauling out buckets of something-or-other for further testing. (Just imagine the toxic stew of vendor machine pastry filling, spilled popcorn oil, stale semen and spermicide, bhang water, and congealed grain alcohol and KoolAid in those buckets.)
NBC repeatedly described ricin as "a component of biological weapons." CBS had the raving ratcheted down to "a potent biotoxin." Now, I'll bet you a subscription to The Journal of Transgressive Post-Feminist Semiotics that upon further testing, the mysterious white powder will turn out to be, not ricin, but paper dust from a printing calculator or the machine that put the quarters in the sleeve. If Osama figured that the best way to kick off the final battle to destroy the United States was to attack a University of Texas sophomore through her change for the washing machine, we probably should feel relieved.
However, you don't need me to point out the obvious. What I have to add is the absurdity of the ricin hype, which we'll apparently have to bury at the crossroads with a silver stake through its heart if we ever want to kill it. During the Weapons of Mass Destruction™ hysteria leading up to the criminal aggression against Iraq, we heard about ricin in screaming headlines week after week. Supposedly it had been found in a train locker in France, in somebody's apartment in England, in the cubicle of a computer programmer in California. The terrorists were coming with ricin to kill us all! The Boston Globe described ricin as a "germ weapon" and after I wrote to them, adamantly refused to run a correction, claiming that Congress had proclaimed it to be one and that was good enough for them. (Seriously. Congress could repeal the law of gravity but that would not cause us all to float off the earth. The Globe also reported that Jack Abramoff "gave generously to Democrats" and refuses to run a correction. Do not believe anything you read in the Boston Globe.)
Okay folks, time to get a grip. Ricin is not a germ weapon, or a biological weapon in any meaningful sense of the term. It is a chemical poison -- just like all the popular poisons of detective fiction since Sherlock Holmes. If you want to kill somebody with ricin, you have to get them to eat it or inhale it, or inject them with it -- just like cyanide, arsenic, atropine. It is "biological" in the sense that it is derived from a plant, but so are most common poisons. It is a "biotoxin" inasmuch as it is a toxin; all toxins are "biotoxins," that's what toxin means, a harmful biologically active substance. It is not especially useful for military or terrorist weapons because it is non-volatile. You could open a 50 gallon drum of ricin in the subway and it would just sit there. Its claim to fame is that it is an unusually potent poison by weight, so the KGB favored it for assassinations, but they could have used other poisons to equally good effect. That's it. It's nothing special. And those field tests are intentionally designed to be highly sensitive at the cost of specificity, in other words they readily give false positive readings.
If the entire country can be provoked to mass hysteria every time somebody finds talcum powder in a medicine cabinet or guacamole spilled on a sidewalk, al Qaeda can just sit back and watch us drown in our own stupidity. Their diabolical scheme is working.
Friday, February 24, 2006
Cleaning out the in-box
Well, I'm back in the real world, from my sojourn in the bowels of the federobble gummint. Let me say that there are still innumerable career civil servants toiling away to do what's right as best they can, but they are wading upstream through rivers of sewage.
Okay.
1. Iraq. With Baghdad locked down, and today being the sabbath, violence has subsided, at least for the time being. While we can still hope that Iraqis will pull back from the abyss, the prospects are dim. The U.S. military stood by and made no attempt to provide security during the past two days, according to all accounts. (I have read the New York Times coverage, and additional coverage is available here and of course, here.) The reason is that they are trying to validate the policy of turning over security to the Iraqi forces. The problem is that there are no Iraqi forces -- the security services that the U.S. has been arming, financing, and training, are simply the militias of Shiite religious parties, in new uniforms. The Sunni Arabs are forced to defend themselves. It has long since become obvious that the U.S. has no discernible or coherent objectives in Iraq, and that the administration is just trying to play for time so as not to admit total failure before the November election. Too late.
2. Environmental Tobacco Culture. Professor Banzhaf, he of the friendly advice to local school board members about sugary soft drinks in the cafeteria, has an interesting take on efforts underway in Canada to ban smoking in most public outdoor spaces. Very few people in the public health community advocate prohibition of tobacco, both because we respect the liberty interests of people who smoke, and because of the counterproductive effects of prohibition of other drugs. However, there has been widespread support for measures, now very widely adopted, to ban smoking in indoor public places such as restaurants, theaters and workplaces, because environmental tobacco smoke is hazardous to non-smokers. As the saying goes, your right to swing your fist ends at the tip of my nose. Outdoors, though, smoke dissipates very quickly and there is no real hazard to anyone who isn't standing right next to the smoker.
Banzhaf, testifying on behalf of an ordinance to ban outdoor smoking in Calabasas, California, offers this rationale:
[C]hildren, as well as some slow adults, will begin to see and appreciate that smoking is no longer the norm to be emulated. Rather, smoking will join gambling, boozing it up, spitting, and certain sex-related pastimes as activities which, while not illegal, should nevertheless be done in private where they do not adversely affect or influence others."
Now this is interesting. It is an argument from the standpoint of public morality -- that allowing the practice to take place where people can observe it is corrupting, particularly of children. We may believe this to be true but there is a catch: this casts smoking in public as a form of expression. While meaning to trump the liberty interest, it actually elevates it by bringing in one of the freedoms we most zealously protect. This is a tough one, for me.
3. Cultural competency in mental health. In case you want to know what I was doing in Rockville, Maryland, it was talking with numerous of my colleagues about this question. To quote a person very close to me, "To try to measure cultural competency in mental health care is to enter an epistemological hall of mirrors." To provide mental health care means to apply diagnostic labels to people and then to try to cure or control the disease which you have declared them to have. That entire procedure can only exist within the context of your culture as a provider. The "client" or "patient" who you are "treating" may very well not believe that any such disease even exists, let alone that they have it, and his or her idea of cure or wellness may be very different from your own.
But you can't just let the client decide what constitutes a good outcome. The result could be highly offensive to society, to your career, or to the client's life expectancy. The culture does impose norms of behavior and wellness. We can criticize them, re-think them, even choose to violate them. But we cannot dispense with them.
Wednesday, February 22, 2006
Brave New World
Okay, here I am in Rockville, MD attending a meeting at the HQ of the U.S. Substance Abuse and Mental Health Services Administration, located in a vast post-industrial office park wilderness.
When you walk in the front door, there is of course a security station, with armed guards and metal detectors. Behind the security station, on either side of the portal leading to the inner sanctum of the building, are two enormous plasma TV screens, on which are displayed, all day long, Fox News.
Oh, and by the way, the same feature is prominently displayed in the lobby of the hotel where we are staying. For whatever it's worth, of course, the hotel (a Hilton) predominantly does business with the federal government. At Logan Airport, through which I passed to get here, the newsstands (owned by Hudson News) all have enormous televisions showing, during all hours when the airport is open, Fox News.
I may talk about the meeting later, but it turns out I was supposed to turn in my visitor's badge when I left the building, which I did not know. You may never hear from me again.
Tuesday, February 21, 2006
Good intentions, but a little it over the top?
It seems that Richard Daynard (with whom I am acquainted) and John Banzhaf, public interest attorneys who battered the tobacco companies into submission a decade ago, are about to sue the manufacturers of sugary soft drinks over the agreements they have made to sell their products in schools. Go for it!
They are also sending out very unsubtle warnings to members of local school boards that if their school districts have participated in such agreements, they could face various categories of individual unpleasantness as a result of coming lawsuits. From Banzhaf's site:
YOUR POTENTIAL INVOLVEMENT AS A PARTY: For more serious is the real possibility that school boards -- and possibly even individual school board members -- will become involved as named parties to these law suits. This could happen in several ways.
FIRST, the bottler defendants could seek to bring the school boards in as necessary parties. They presumably would argue that it is the school boards -- entities charged with the primary responsibility for protecting the health of the children -- which made the final decision to provide students with sugary soft drinks during school, and that the school boards are therefore an essential part of any resolution of the problem.
SECOND, perhaps as the result of pre-trial discovery of previously unknown facts -- e.g., secret memos or minutes of school board meetings, "wining and dining" of school board members or other benefits to them, etc. -- the pleading by the initial plaintiffs could be amended to include new parties such as school board members.
THIRD, other parents who believe that the school board and its members are at least equally at fault -- including some who might wish to run for school board membership and/or have other agendas they wish to promote -- may bring new law suits against the school board and/or its members, and then probably seek to have these new law suits consolidated with the existing law suits (i.e., those by the initial plaintiffs against the bottlers).
YOUR POTENTIAL LEGAL LIABILITY: School boards -- and in some cases even individual school board members -- could be sued and potentially held liable under a variety of legal theories ("causes of action"). Some of the major ones are discussed very briefly below. . . .
And it goes on from there, and just gets scarier. In other words, these lawyers want to scare the school committee members straight -- get the toxic slurm out of your public schools, or you will be sorry.
Maybe this is right, maybe it's called for, maybe it will be effective. Or maybe it's counterproductive bullying of ordinary citizens called to public service who suddenly find themselves in over their heads, and it's just going to lend credence to Republican trial-lawyer bashing and give the soda companies an opportunity to make themselves look like they're the kind and gentle dogs in this fight.
What do you think?
Promises, promises
So where is the legislation to ban animal-human hybrids? I am prompted to ask because I'm about to go to Maryland for a Center for Mental Health Services grantee meeting, and that reminds me of something else -- Compassionate Conservatism was supposed to mean eliminating inequality for Americans with disabilities, particularly those associated with mental illness.
Remember the President's New Freedom Commission on Mental Health? One of the first things the new administration did was set up this commission, which made all sorts of recommendations to heal the fragmentation of services for people with mental illnesses, provide access to care for everyone who needs it, support recovery and independence, yadda yadda yadda. It turns out that the only real world manifestation of all this goodness that even got close to happening was a proposal to screen all the schoolchildren in America using a protocol developed by drug companies, so as to get them all on whatever pills Pfizer thought they should be taking. There was a great hue and cry but nothing came of it anyway because it would have cost actual money.
CMHS has just issued a new policy statement about recovery -- how everybody with mental illness is entitled to the supports they need and the opportunity to live independent, full lives, etc. That is truly charming. Meanwhile funding for CMHS is being cut.
There is not one single area of public policy -- not one, zip, zilch, nada, bupkis, zero, nothing -- in which this administration is not hypocritical, dishonest, corrupt, and just plain wrong. The pathological liar in the Oval Office says that society is judged by how it treats the most vulnerable among us, by which he means the brain dead and the embryonic. People who are conscious, and who are troubled and suffering, don't mean shit to him. Actually I sincerely doubt he cares about the blastocysts and the vegetative either, or anybody or anything except his own power and the adulation of sycophants.
I hope to be able to post from the road, but it may turn out to be a problem. If I'm absent for a couple of days, you'll know why, but I'll catch up when I'm back.
Sunday, February 19, 2006
The No-Exit Strategy
A lot of bloggers make their living by dropping in on the opposition and mocking them -- you know, Atrios and the Wanker of the Day, that sort of thing. As you know, I always try to stay positive, stay on the sunny side, look forward not back. But what the heck, I said to myself, I wonder what Pat Robertson is up to these days?
It turns out he has an Iraq exit strategy. And you can help! That's right, every Christian American can do his or her bit to bring our troops home. Ahh, there is a small catch -- you have to "join the community," which means that Pat will ask you for money -- but that's really just an added benefit, since you will have so many ways to give and so many opportunities to be relentlessly asked. Not only that, you get a health benefit -- a chance to learn all about Pat's Age Defying Antioxidants!
Here's how it works:
Here is the Biblical Exit Strategy
We are asking thousands of churches and individuals to adopt the newly-elected Iraqi leaders by name for six months of weekly prayer support in three areas:
* For Safety: They and their families must survive the many attacks that will come.
* For Wisdom: They must have the wisdom of God to rebuild their government and nation.
* For Courage: To persevere in serving Iraq until the job is done.
Within three months, we intend to send each adopted Iraqi leader a list of hundreds -- perhaps thousands -- of Christians and churches in America and worldwide praying for them and their families by name for 180 days!
* This kind of sustained prayer for Muslim leaders may never have been done before in Church history! This is a wonderful way to love Muslims with God’s love!
* 180 days of prayer could empower those leaders to turn Iraq 180 degrees toward peace and stability -- hence Back Iraq 180!
You'll get regular e-mail updates on prayer needs from Iraq, along with regular updates on Pat's need for money. And the best part is, it's bound to work! I mean, how can history possibly defy the power of prayer to the Christian God?
I've only got one question -- if God can fix this thing, why is he waiting around for Pat's followers to pray for it? Isn't that kind of unfair to all those people who are getting blown up and shot in the meantime? Just a thought. Plus I have another question -- why bother to take Pat's age-defying antioxidants when you can just pray for youthfulness?
Administrative note: I'm doing Today in Iraq and Confined Space today, so that's all you get from me here for a while. But do check out our blog partners.
Saturday, February 18, 2006
Not a family guy
I'm sure y'all have heard more about it in the rest of the country than you might like to, but here in Massachusetts its been wall-to-wall, non-stop, all Neil Entwhistle all the time on the TV and in the newspapers. That's the fellow who (pending a unanimous finding by a jury of his peers) appears to have shot his wife Rachel and their infant daughter in the marital bed before fleeing to his native England. (Unlike Harry Whittington, who had the good grace to apologize to Dick Cheney, Rachel's parents have yet to apologize to Neil.)
Anyhow, as with all such media feeding frenzies, some cultural criticism seems to be called for here. Although the rate has been declining, about 1,200 women are murdered by their husbands, ex-husbands or boyfriends each year in the U.S. Women kill their male partners less often, about 300 times a year. Either way, guns are the most popular method. You can take a look at the trends in California here. Discussion of the reasons for the recent decline -- mostly lesser exposure in that divorce is more common and people are more often single, as well as improved access to domestic violence services -- is offered by some learned professors here.
So okay, out of thousands of man-kills-family stories, why does this one get the OJ treatment? We know why OJ got the OJ treatment, but this one featured a non-famous protagonist and no race relations implications. It did, however, happen in an affluent suburb in a family of middle class origin, complete with pictures of the victims just about glowing in the dark, and the expensive looking home with the faux-brick facade. (Actually, they were broke, and the house was rented, but the picture still looked good.)
Reporters, as a class, are intellectually lazy and irresponsible. That's all there is to it. The profession as a whole is in a disagraceful state. What is most disturbing is that they don't seem to realize that they have lost the respect of the public, and they aren't making the slightest effort to win it back.
Friday, February 17, 2006
The doctor will not be in . . .
The American College of Physicians, which is the appropriately general name, I suppose, for internists -- primary care doctors for adults -- foresees its own extinction. The Impending Collapse of Primary Care is the alarming title of their recent report on the state of the profession.
Sure, there's self-interest involved -- they want to get paid more, or work less, or a little bit of both -- but the fact is, fewer medical school graduates are going into primary care, and more primary care docs are getting out. The major complaints are not new -- the alarm bells have been ringing since I first studied health care policy 20 years ago, but we've just been going backwards. Medicare is extremely important in this story, but so is private insurance. Health insurance underpays for primary care physicians' time spent with patients, and the money flows toward diagnostic procedures and technical interventions.
Many of you probably are aware of the recent New York Times article that noted that diabetes management programs in New York City failed financially, even though they were successful medically, because insurers wouldn't pay for the time spent with patients to support them in taking care of themselves and preventing complications, whereas they have no problem at all with paying $30,000 for amputations.
Here are a couple of points from the ACP report:
A recently-published study of the career plans of internal medicine residents documents the steep decline in the willingness of physicians to enter training for primary care. In 2003, only 19 percent of first year internal medicine residents planned to pursue careers in general medicine. Among third-year internal medicine residents, only 27 percent planned to practice general internal medicine compared to 54 percent in 1998.
snip
The declining interest in careers in primary care is important because the collapse of primary care will result in higher health care expenses and lower health care quality:
• When compared with other developed countries, the United States ranked lowest in its primary care functions and lowest in health care outcomes, yet highest in health care spending.
• Studies have shown that primary care has the potential to reduce costs while still maintaining quality. Not only does early detection and treatment of chronic conditions play a vital role in the health and quality of life of patients, but it can also prevent many costly and often fatal complications when illnesses such as diabetes and cancer are diagnosed at a later stage. As expert diagnosticians, providing patient-focused, long-range, coordinated care, general internists play a significant role in the diagnosis, treatment and management of chronic conditions. It has been reported that states with higher ratios of primary care physicians to population had better health outcomes, including mortality from cancer, heart disease or stroke.
• States with more specialists have higher per capita Medicare spending. An increase in primary care physicians is associated with a significant increase in quality of health services, as well as a reduction in costs.
. . . If they do say so themselves. But they're right. Medicine ought to be about taking care of people, and doctors who do that need to be valued, and paid for it.
Enough already
If Dick Cheney wants to shoot his pals, that's fine with me. Have at it!
I'm much more worried about the tens of thousands of strangers who he has maimed, tortured, and murdered. But that's just me. Evidently the rest of the world, including Atrios, Josh Marshall, Matthew Yglesias, and the whole gang, have the opposite opinion.
Maybe we should consider talking about something else. Just sayin'.
Thursday, February 16, 2006
Department of How could I have missed this?
I believe I had something to say last year about the vicious cuts in Missouri's Medicaid program, which immediately threw 90,000 poor people -- elderly, disabled, and families with children -- off the rolls, and cut benefits to 300,000 more, including, get this, breathing equipment. Of course hospitals are stuck with the bills for people who can't pay, and the state loses federal matching funds. But I missed two kind of important points at the time. The first is Governor Matt Blunt's concept of Christian morality. Here's from the NPR story last May:
The proposals have opened a moral schism, with some preachers expressing outrage, but the governor, a devout Christian, defends the cuts as morally correct. Gov. Matt Blunt says not cutting Medicaid would force him to raise taxes -- and in his eyes, raising taxes is wrong.
That's from the Gospel According to Saint Pat Robertson, of course.
What I also missed is that they also voted to eliminate Medicaid entirely by 2008. Now that's really getting Christian on the people's asses. According to Community Catalyst, however, the devil stalks Missouri -- they just aren't good Christians after all:
Despite the rhetoric from conservatives, polls show that these cuts are not popular with the public. A recent poll of 800 likely voters commissioned by the St. Louis Post Dispatch and KMOV-TV found that 22% of voters rated providing Medicaid to the poor and disabled as the most important issue facing Missouri, second only to education (25%). 64% thought the cuts made to Medicaid were "too severe". (St. Louis Post Dispatch, January 21, 2006).
Missouri hospitals have been pushing an initiative for a tobacco tax, but the money would not go to support Medicaid, so a coalition has formed to save Medicaid in Missouri through the tobacco tax. That may be better than nothing but the last thing the Satan worshippers in the Show Me state should want is for Medicaid to be dependent on healthy sales of cigarettes. Meanwhile, all I can say is, if Jesus Christ was alive today, he'd roll over in his grave.
As if I didn't have enough to do . . .
Nevertheless, I'm honored to have the opportunity to join Revere of Effect Measure in holding down the fort at Confined Space for Jordan Barab while he takes a week's vacation (whatever that is -- some sort of voluntary absence, as I understand it.)
Jordan has been a leading web voice on occupational safety and health for a long time now. I can't fill in adequately, but I'll do my bit to keep the seat warm. Hope you'll all check it out.
Wednesday, February 15, 2006
Repost (mostly): An Influenza primer
This is largely a repost from last year, but it turns out we have some readers new to this site who are interested in knowing some of the basics, so here goes.
There are three major sub-types of influenza virus. B and C don't cause big problems but type A is a major drag on the human condition -- in part because it's also a bummer for pigs, horses, Flipper and Shamu, and birds, which means we can't get rid of it. Influenza A replicates sloppily, which means it is constantly mutating. These small mutations are why the flu shot you got last year won't work this year. But the even worse part is that the virus can swap whole gene segments.
That's bad because the virus has a protein called haemaglutinin (HA) that sticks out from its surface and gets it into cells. There are 15 known major sub-types of HA, in virus that infects birds, but only 3 sub-types are known to have been prevalent in the human population -- called H1, H2, and H3. So, if a variety with, say, H5 were to develop the ability to infect humans, we'd be up a very thick and sticky creek, because nobody on earth has any immunity to H5 influenza.
Starting in 1997, there have been recurrent outbreaks of an H5 strain (specifically H5N1, with the N designating another protein called neuraminidase, which is less important to infectivity) in domestic and wild birds in Asia, which in at least two countries, Vietnam and Thailand, have infected people. (Note: Since I wrote this, of course, there have been human cases in China, Turkey, Iraq and Indonesia, as well.) This strain causes very severe disease and has killed young and healthy victims. It has also shown (so far) limited ability to be transmitted from person to person. H5N1 is now firmly entrenched in Asian bird populations and it's showing up in all sorts of unexpected places -- even tigers, which is really novel. Many experts believe it is likely only a matter of time before an H5N1 strain hits on the right combination of mutations to become highly infectious among Homo sapiens, and then, Kapow! -- by which I mean millions of seriously ill Americans (not to mention the rest of the world), severe disruptions to international commerce, an overwhelmed health care system, and, if enough people are sick at once, possible break downs in public services causing all sorts of collateral damage.
(To clarify, which I probably did insufficiently the first time, the idea is that the basic structure of the H5 haemagluttinin spike remains the same, but the virus undergoes other, small mutations that enable it to pass efficiently from human to human. This can happen either by random mutation, or by genetic recombination with other viral strains in dually infected humans or even swine.)
Other bloggers are on the case regularly, so that's all I'm going to have to say about this for now. Except that, in conclusion, our wartime President has diverted vast quantities of public health funding and planning to the threat of bioterrorism, which has now become largely synonymous with public health emergency preparedness. This has meant not only immediate misdirection of government resources, but also a cultural blind spot. Nature is still out there folks.
And, as a further update, since I wrote this our wartime President finally noticed the problem. The response, however, has been inadequate and largely inappropriate. I commend interested people to the Effect Measure blog, where this is covered very closely by a real expert, which I'm not. The last really major flu pandemic, in 1918-19, was also an avian flu. It decimated troops fighting WWI, and probably contributed to the end of that conflict. Lesser pandemics have happened since.
Further addendum: I realize that I also need to explain that, while ordinary seasonal flu and pneumonia mostly kill frail elderly and immunocompromised people, past pandemic flu strains, and H5N1 so far, have preferentially killed young and healthy people. The reason seems to be that the killing mechanism is a hyperactive immune response, a so-called "cytokine storm" (cytokines are molecules that cells use to signal each other, which are essential to immune response) in the lungs, that causes the lungs to fill with pus and fluid so that the victim drowns. Younger people, with more active immune systems, are actually more at risk than us semi-codgers. The only way to keep people alive through this is with mechanical ventilation, but there aren't nearly enough ventilators to go around. Sorry for the major bummer folks, but y'all need to know. This may or may not happen, but it's a legitimate concern. Probably fewer than 5% of sufferers will actually die, but that's still potentially a lot of people. And 30% of the population or so will become ill, if the event is like 1918.
The Evil Chemical
Okay, I did my duty and watched the Frontline program on meth last night. It's basically factually accurate, with a couple of significant oversimplifications, but very shallow on analysis. That's forgiveable, I suppose, since they had to cram the basic into 50 minutes, but they did leave some important stuff out.
First of all, methamphetamine is not just something that people cook up in illegal labs out of cold pills. It is an FDA approved pharmaceutical which was first sold under the brand name Methedrine. Lenny Bruce's doctor gave him a prescription for injectable Methedrine ampules, which ultimately killed him. As far as I know methamphetamine is seldom if ever prescribed in the U.S. any more, but its cousins dextroamphetmine (Dexedrine), amphetamine, and Adderall are still approved for treatment of Attention Deficit Hyperactivity Disorder, and narcolepsy.
The Frontline piece noted the correlation between the purity of meth available on the street and indicators of the prevalence of addiction. It implied that when the available drug is less pure, it is less addictive, but that is highly doubtful. If an intoxicant is less pure, people will simply use more of it (viz. "light" cigarettes). In fact, the purity of the available street drug is probably just a surrogate for general availability. If it's harder to get, then probably fewer people will start using it.
But that's where the real problem with the story begins. It told of meth's seemingly relentless march from the west coast to the east, but the fact is meth still hasn't made it to most of the eastern U.S. -- it's a problem in the economically undeveloped, rural southeast, but not in the northeast. And on its way across the country, it didn't particularly come through Chicago and St. Louis, it came through rural areas. The exception is that there is a sub-culture of meth use among gay men in some cities.
Amphetamines were, and as far as I know still are, commonly used by truck drivers on long hauls: (And if you give me weed, whites and wine, and you show me a sign, I'll be willing, to be moving. "Whites" are Dexedrine.) Also used by college students cramming for exams. I don't know about the truck drivers, but the college students seldom become addicted.
The point of all this is that drug abuse and addiction aren't caused directly and simply by the chemicals themselves. These problems arise from a confluence of culture, economics, and individual psychology -- the latter itself influenced by the first two. Most people who ever use an illicit drug, including amphetamines, do not become addicts. That may not be true of tobacco but there was, until recently at least, very strong cultural support for tobacco use. Back in the '60s, when hippies were using hallucinogens and marijuana, meth -- speed -- had a very bad reputation in hippie culture and no respectable hippie would go near it. "Speed Kills," was the slogan. Truckers and bikers did meth.
Today, it's still part of rural culture. As you could have deduced from the Frontline piece, although they never connected the dots, one factor in the problem is the lack of economic opportunity in much of the rural U.S. People start cooking meth for the same reason they join the Army -- there's no other way to make a living. And people start using it, and get hooked, for more or less the same reason -- they have nothing better to do with their lives. Deep psychic pain can also be a major reason. As you could also pick up from the Frontline piece, if you were paying close attention, people who manage to give up the drug usually haven't begun to solve their problems -- they still need to go back and deal with whatever it was that they were running away from in the first place.
It does happen to be true that meth is one drug of abuse for which relatively effective supply side restrictions may be possible. But the problem of drug addiction is not fundamentally about supply. And that's where the Frontline documentary came down wrong, in my view.
Nature is still the boss
I haven't had a whole lot to say about the whole bird flu thing because a) you can read all about it on Effect Measure if you enjoy the feeling that death, doubt and doom loom; and b) who the hell knows what's going to happen? I try to steer clear of news of the future.
However, given that I'm now holding down the public health and Iraq portfolio for my friends at Today in Iraq, I do need to acknowledge the situation there. We've heard about the appearance of the H5N1 virus in Kurdistan, but now it's shown up in the poorer, less orderly south of the country and the authorities are worried, big time. Buried in Bushra Juhi's daily news round-up for the AP is the following (which is getting zero headlines as far as I can tell):
Iraqi authorities, meanwhile, have declared a bird flu alert in the southern province of Maysan and called for security forces to prevent people from carrying birds in and out of the area, health officials said Wednesday.The alert is the latest measure taken by Iraqi health authorities to combat the deadly H5N1 bird flu strain following last month's discovery of the country's only confirmed case of the disease in a human.
Minister Abdel Mutalib Mohammed declared the alert after birds suspected of having the disease were discovered in Maysan, a major southern trade route in Iraq, said Dr. Ibtisam Aziz Ali, spokeswoman for a government committee on bird flu.
Mohammed said the government has to "totally close" Maysan using Iraqi soldiers and police and carry out culling of poultry. He didn't elaborate further on what steps would be taken to close the province.
Mohammed held talks late Tuesday with local health authorities and tribal sheiks in Amarah, 180 miles southeast of Baghdad, to brief them on the bird flu threat and government measures to combat it.
"The disease has apparently spread among local birds, not migratory birds," Mohammed said. "I have seen five centers where infections have been detected by rapid laboratory testing. Now we have declared a state of health alert."
Maysan includes some of Iraq's famous marshlands, and U.S. and U.N. officials fear the deadly disease could spread rapidly if it reaches the area rich in bird life.
Bird flu has killed at least 91 people since 2003, according to the World Health Organization. Almost all the human deaths have been linked to contact with infected poultry, but experts fear the H5N1 virus could mutate into a form that spreads easily among people, possibly sparking a pandemic.
Tests are being carried out at a WHO-approved lab in Egypt on samples taken from about 10 suspected human cases in Iraq, including the deceased uncle of a girl who died Jan. 17 of the disease in Iraq's northern Kurdistan region.
Now, it is possible that the ministry of health is overreacting. They have not taken similar measures in Kurdistan but that may be for political reasons -- the Kurds rule Kurdistan and I'm quite sure that Abdel Mutalib Muhammed is irrelevant there, whereas the Shiite government does have at least de facto authority in Maysan. But they have a very difficult challenge in that the region is marshy, undeveloped, and insular. There is no way the government can really understand what's going on there, let alone control the situation, which may account for the decision to try to isolate the entire region. Of course it is hopeless -- they can't stop wild birds from flying, and they can't stop people from traveling and trading.
You can look at a map here. . You'll see that the region is on the Iranian border, bisected by the Tigris, and full of swamps. The government cannot possibly seal it off, or seriously hope to control what happens inside.
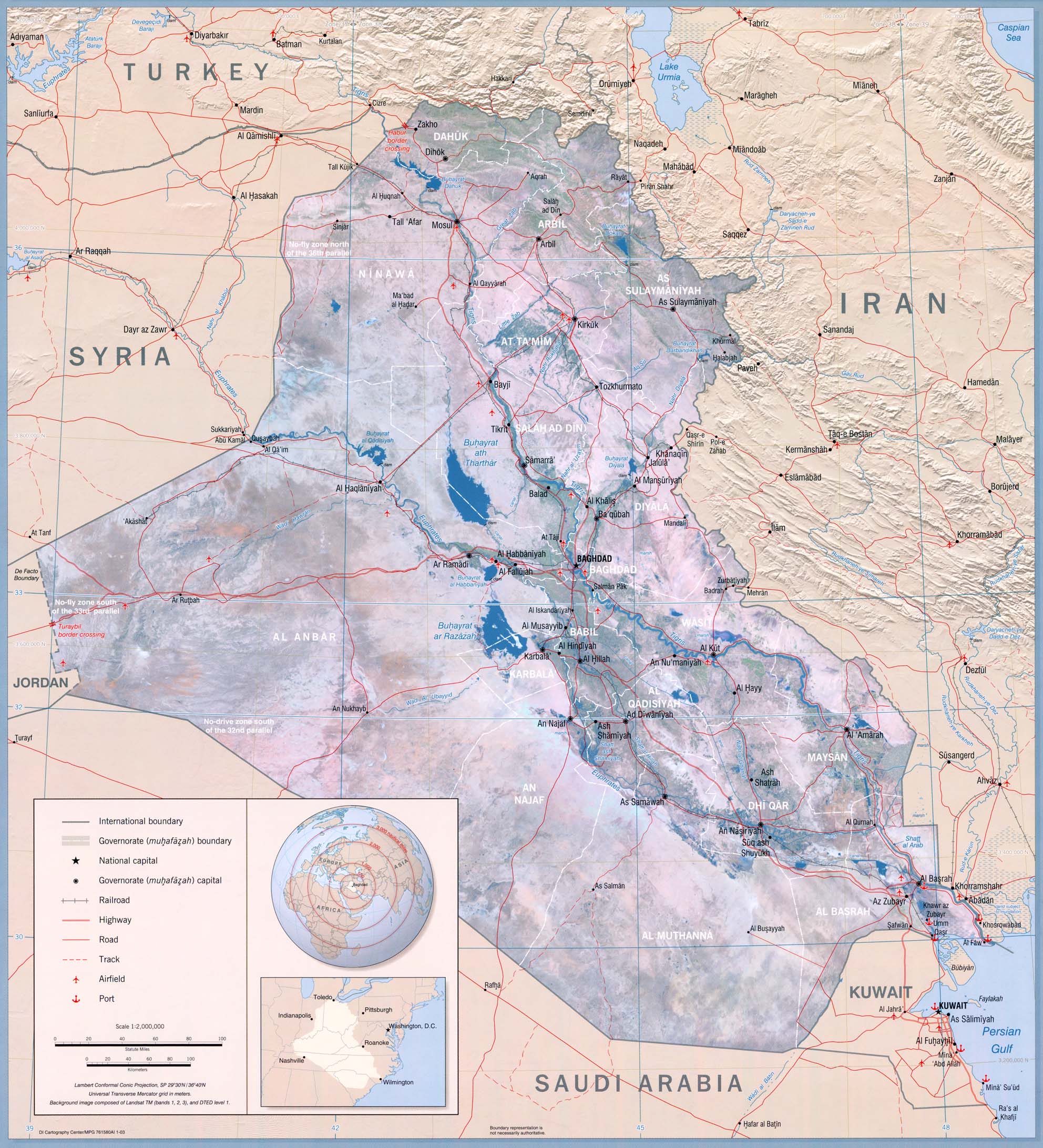{kind=link}
If a human influenza pandemic should happen to begin in Iraq, the consequences for history may be profound. For one thing, of course, it will seriously set back the effectiveness of the military occupation for a considerable time. The insurgency, which is far less rigidly organized and hierarchical, will presumably be much less affected. It will also quickly spread to neighboring countries, and may contribute to political instability with consequences that no-one will predict.
My point in mentioning all this is not that I necessarily expect anything in particular to happen -- I just don't know. It is rather to point out that the hubris of the neocons, in thinking that they could seize control of history, was utter folly. They didn't understand Iraqi society, political science, or for that matter, nature. We're still a part of it.
Tuesday, February 14, 2006
Why don't they tell us the good news?
The population of Iraq is about 24 million, just a tad more than the population of Texas. Imagine that in Texas, several acres in the center of the capital city, including the capitol building and government offices, are surrounded by a 12 foot high blast wall, and that citizens are forbidden to enter the zone to meet with their representatives or officials of state agencies, or to observe legislative or court proceedings. The state is occupied by 140,000 Russian soldiers, who travel in armored convoys and shoot 50 caliber automatic rifles at any vehicle that gets close to them. Hardly any of them speaks a word of English.
The government is controlled by evangelical protestants, whose police work closely with the Russian soldiers. The evangelicals live in separate neighborhoods from people of other faiths. Routinely, Russian soldiers surround non-evangelical neighborhoods, while the evangelical police break down the doors of every house, force the inhabitants to kneel in the front yard, and ransack the homes. On each occasion, they haul away a dozen or so young men to secret prisons, where they join thousands of others who are held without charges, who have no access to lawyers or the legal system, and who no-one is allowed to visit. On a typical Friday:
- A car bomb kills 9 people at a Catholic church in Lubbock.
- A Texas Ranger is killed and 3 are injured by a roadside bomb in Dallas.
- A car bomb in Waco kills three civilians.
- Gunmen kill a government official in Galveston and kidnap another.
- A roadside bomb kills a police lieutenant and injures a police captain in Crawford.
- A Russian helicopter fire two rockets into a Jewish neighborhood in Houston, killing six members of a family. The government claims the dead were all insurgents.
- A gunfight between unknown militants and Russian and Texan forces near Texas Stadium results in four injuries.
- Gunmen killed a policeman in Huntsville.
- The kidnappers of a Russian journalist threaten to kill her unless the Russians release all the Texan women they hold in prison.
- Gunmen kill a traffic policeman in College Station.
- Gunmen killed a police sergeant on patrol in Nacogdoches.
- A roadside bomb kills a civilian in Fort Worth.
On this day, as on most others, a couple of dozen people are kidnapped for ransom. It is unsafe to travel on the highways, and bodies turn up with their hands bound and signs of torture in vacant lots every day. Most of the state has electricity for only 4 hours a day, and most Texans have contaminated drinking water. The unemployment rate is 60%, and 10% of children are malnourished. Most people depend largely on government rations for food.
Vladimir Putin complains constantly that the news media aren't covering all the good news from Texas.
Monday, February 13, 2006
Straight Shooting
For some highly mysterious reason, CDC has no links on its web site to information specifically about firearm related injuries. That's not to say you can't find any, but you have to root around in other categories, such as homicide and suicide, meaning there is no evident way to get information on unintentional gun-related injuries. Hmm. Maybe I should get interested in other topics, such as global warming or mercury pollution. I'm sure the federal government has lots of good info about that.
Meanwhile, there's Medline. The latest national data I could find on hunting injuries is from 1996. Sinauer, Annest and Mercy, in JAMA (12 June, 1996) estimated the national incidence of unintentional, non-fatal firearm-related injuries from June 1, 1992 through May 31, 1994, using data from a network of sentinel injury surveillance systems in selected hospital emergency departments around the country. They estimated EDs in the U.S. treated 34,385 people for such injuries during that two-year period. (About 1,500 people die from unintentional gunshot injuries in the U.S. each year.)
12.3% of these were hunting injuries. Smith, Wood, and Lengerich, reporting in the Journal of Trauma, Injury, Infection and Critical Care in March, 2005, analyzed hunting injuries in Pennsylvania from 1987 to 1999. That state requires that hunting injuries be reported and investigated. Turkey hunters had the highest incidence of injuries per 100,000 (5.5 in the spring, 7.5 in the fall) followed by pheasant hunters (4.0). Most deer hunting injuries were due to poor skill on the part of the shooter, but the vast majority of bird hunting injuries were due to poor judgment.
Interestingly, the rate of injuries goes down sharply with the age of the hunter. Except for turkey hunters, there were hardly any injuries caused by hunters over 50 yars old. 60% of pheasant hunters who shot people shot members of their own hunting party. It's uncommon for bird hunters to shoot people, especially older, more experienced hunters, but when it happens, poor judgment is almost always the cause.
Well, that's no surprise. When you also get to decide what countries to invade, it's a big problem.
The Cost of War
Many people have no doubt read accounts in the general press of the study by Pizarro, Silver and Prause in the Archives of General Psychiatry entitled "Physical and Mental Health Costs of Traumatic War Experience Among Civil War Veterans." You can read the abstract here, although as per my usual gripe the full article is subscription only.
It obviously isn't news that combat is bad for you, even if you don't suffer serious physical injuries. From the author's literature review:
WAR IS PARTICULARLY traumatic for soldiers because it often involves intimate violence, including witnessing death through direct combat, viewing the enemy before or after killing him, and watching friends and comrades die. . . .Many investigators have examined the mental health consequences of exposure to war trauma and found substantial postwar psychiatric difficulties among veterans. Research has also linked war trauma and physical health outcomes, including an increase in negative physical symptom reporting, chronic illness, and death. Traumatic war exposure has also been linked to specific self-reported and objective health problems, such as cardiovascular disease and hypertension and gastrointestinal (GI) disorders.
So what's new in this study? To me, what is most interesting about it is that exposure to greater psychological trauma -- the percentage of a soldier's company killed, in particular -- was associated with physical symptoms, both cardiac and gastrointestinal, but not with so-called "nervous disease" (what we today would call mental disorders) alone, but only for soldiers who were not physically wounded. As a matter of fact, soldiers who were physically injured were less likely to suffer from these symptoms than soldiers who were not, although wounded soldiers were more likely to suffer from nervous diseases.
Back in the 19th Century, the concept of Post Traumatic Stress Disorder had not been developed. Possibly some of these soldiers who were not diagnosed with a "nervous disease" would have gotten that diagnosis today. In any event, what this says to me is that the emotional trauma of war can manifest over the life course in physical symptoms. We don't, obviously, have angiograms EKGs or CT scans or endoscopies of these soldiers. We don't know what physical diagnoses they might receive were a time machine to bring them to us today. But I doubt these symptoms were purely psychogenic. The brain is a physical organ, the nervous system affects the functions of other organs including the secretion of hormones. Psychological damage is a kind of physical damage. This undoubtedly helps to account for some of the unexplained ailments of modern veterans as well.
Sunday, February 12, 2006
What is
On Darwin's birthday, I presume everyone will be talking about evolution. So I will talk about cosmology.
A few years back, Sky and Telescope magazine ran a contest to come up with a better name for the Big Bang. I didn't bother to send in my entry because I thought it was so obvious they'd get it from a million people. Evidently they did not -- they declared no winner, and we're stuck with the Big Bang. But there was no bang, nor was it big. The beginning was infinitely small. It was the Initial Singularity, the IS. What name could be better than that? The IS Theory.
Cosmologists deduce the IS by running the expansion of the universe backward. Actually an infinitely small, hot and dense initial state, as such, can't be proved, but a state so dense that the structure of space-time break down is an impenetrable barrier to our understanding of what may have existed (if that is the word for it) before the beginning. When cosmologists talk about the universe, they mean everything that can be observed, because that is the subject matter of science. "Observable" doesn't mean we can see it or hear it directly, of course, but that we can demonstrate that it must be based on what we can apprehend with our senses, through the application of reason.
This universe evolved by expanding from the IS, cooling and attenuating in the process. By creating conditions in particle accelerators similar to those that must have existed in earlier epochs, physicists have been able to deduce a great deal about how the universe must have changed through time. Early on, elementary particles condensed from the intense energy. Gravity, building on random fluctuations in density, gathered matter into galaxies, and within the galaxies, into stars. The first generation of stars consisted only of hydrogen, but heavier elements syntehsized in the stars through nuclear fusion. When stars of the first generation exploded in novae, they spewed these heavier elements into interstellar space, to be incorporated into the gas clouds that gave rise to later generations of stars, and condense into planets. Now here we are.
This universe is not infinite, in time or space, but it is so much older and so much larger than the biblical cosmos that the difference in scale is incomprehensible. The scientific cosmos is troubling to the human spirit. People call it "pointless," and "meaningless." What they mean by that, I think, is that they want people to be important in the scheme of things, and that is precisely what religious myths provide. God is preoccupied with humans. God insists on being worshipped, God intervenes to order human affairs, God wishes to have communion with people. Religious cosmology puts humans at the center. It's arrogance and self-importance is satisfying to people.
Well too bad. In the universe -- just the observable one, never mind what might lie beyond -- we are as close to nothing as we can imagine. There are more than 100 billion stars in our own galaxy, and something like 100 million galaxies in the observable universe. The IS happened more than 13 billion years ago, the earth formed 4 1/2 billion years ago, and we've been here, in more or less our present form, for maybe 250,000 years. All of this is proved beyond any doubt. Look through the telescope. But to most people, it just doesn't feel good, and on that basis, they refuse to believe it.
So how can we feel better? The answer is humanism. We aren't the center of the universe, we aren't the crown of creation, we are nothing -- except to ourselves. Let us set out, in this vast darkness, to become what we can be.
Friday, February 10, 2006
An idea whose time may not have come
CDC estimates that about 25% of Americans who are HIV positive don't know it. It's very important that as many infected people as possible learn their status, so that they can obtain medical care which may slow the progression of the disease before they become symptomatic, and so that they can avoid infecting others. When a test for HIV first became available in 1985, legislation required that it be given only with informed consent. People who told their physicians that they engage in high risk behavior, or who presented for STD testing or with substance abuse problems or other indications of risk at clinics or social service agencies might be urged to consider testing, but it is illegal under most circumstances to test people without their knowledge and permission. Legislation in most states, and CDC guidelines for testing that it funded, required specific counseling protocols before people had blood drawn for the test, and when they were given their results.
The rationale for universal, elaborate pre-test counseling has weakened over the years, as the stigma and discrimination associated with HIV have lessened, but there continue to be good arguments for providing post-test counseling, particularly for people who test positive. Learning that one is HIV positive can be quite traumatic. Some people react with denial, and don't seek medical care or try to change their risk behaviors for weeks, months or years. People may have an addiction relapse, or exacerbation of their substance abusing behavior. They may become depressed. Post-test counseling aims at making sure people are connected immediately with services such as medical care, case management, emotional support, help deciding how and when to tell others, and the opportunity to cooperate with partner notification programs.
In order to increase the proportion of people who know their HIV status, testing is now recommended routinely for pregnant women, and efforts are being made to encourage screening of the general population through routine primary care. For people who test negative under these circumstances, there doesn't seem to be any particular reason to provide substantial counseling. There is still a good argument to be made for counseling individuals who sought out testing due to a known exposure risk, so that they don't take the negative test as a license to continue unsafe behavior.
Last year, the OraQuick HIV test, manufactured by OraSure Technologies, went into widespread use. It's an important advance because it produces a result within 20 minutes, unlike previous tests that required people to come back on a later date to get their test results. Unfortunately, about 30% of people do not return. Rapid testing is not quite as specific as the laboratory tests, so a positive result is reported to people as an indication that they may be infected and still need a confirmatory lab test. Nevertheless, they are still there to be counseled and measures can be taken to greatly increase the likelihood that they will remain in contact with the test site to get their confirmatory results and be connected with appropriate services.
Since 1996, home test kits have been available, but they require the user to send a blood sample to a laboratory and receive the results by telephone. While anonymous telephone counseling is certainly inferior to face-to-face counseling in settings where backup services are immediately available, FDA approval was enough for the kits to be marketed, even in states that objected. While some people are sanguine about this, on the basis that there hasn't been any reported increase in the rate of suicide associated with home testing, I would say that we really don't have any information about how people respond to getting positive results over the phone and whether this is really such a great idea.
But now OraSure wants to market a rapid test over the counter, which would enable people to read their own test results at home without having to talk about it with anyone. Alexi Wright and Ingrid Katz, writing in the New England Journal of Medicine (Feb. 2 -- subscription only) seem to think this is just a terrific idea, as did 18 out of 20 people who spoke at an FDA panel to consider the application. I am not convinced. We need evidence to show that this is not going to be harmful to people.
In addition to the emotional and behavioral risks I have mentioned, the OraQuick test has been associated with clusters of high rates of false positives. If the problem of false positives is resolved, there now seems a good chance the FDA will approve the rapid test for home use. I'm afraid we'll learn about the negative consequences after the test goes to market, as we have with so many drugs. If this is going to happen, it should be done on a small-scale, experimental basis in limited markets, so that we can make a decision based on evidence, not commercial interest.
Mass Murder
We hear it all the time: Al Qaeda killed 3,000 Americans. Actually, the official death toll from the Sept. 11, 2001 attack is 2,967, not counting the 19 hijackers. Among the dead were at least a couple of hundred people who were not U.S. citizens, although I have not been able to find an exact count.
As of this writing, the total of U.S. military deaths in Iraq is 2,267. This does not include people who committed suicide or died as a result of substance abuse or violence after returning home. We know of some publicized instances, but no-one is counting. Military deaths for other coalition partners total 204, for a total death count of U.S. and allied troops of 2,471.
No-one has done a comprehensive count of deaths of civilian "contractors" (many of whom were actually mercenaries, but others of whom were truck drivers and other ordinary workers), but ICCC has been able to compile information on 310 of them, of whom 124 were American. There have also been several American journalists killed in Iraq, and others from various allied countries.
The rate at which U.S. soldiers and Marines have been dying in Iraq this month is 2.6 per day, so far, the highest since November. It is likely that the total number of Americans killed in the Iraq war will exceed the number killed by the Sept. 11 attack before summer. I wonder if anyone will note that symmetry.
Of course, as General Franks said, "We don't do body counts." Nobody has bothered to count the Iraq civilians killed by U.S. and allied forces, or the thousands of conscript soldiers killed in the initial invasion, or Iraqis who have died from malnutrition, lack of health care, and the collapse of public order. As we have noted before, the best available evidence is that the total is something like 200,000.
Draw your own conclusions.
Thursday, February 09, 2006
You can't take it with you
I've been asked to comment on the new rules which make it more difficult for people to qualify for Medicaid who have transferred assets to their heirs in recent years. This is a tricky issue.
Very briefly, because I think most of my readers already understand the gist of this, just about everybody who's 65 or older (or disabled with certain restrictions), is eligible for Medicare. Ubfortunately, Medicare does not pay for long-term care in a nursing home, or other forms of so-called "custodial care" that people might receive through home care or adult day programs. Custodial care basically means services that aren't medical treatment -- feeding, bathing, dressing, protection from wandering and self-injury, social and intellectual stimulation, etc. Furthermore, even if a person needs hard core medical services, in a skilled nursing facility, they aren't covered for longer than six months.
Alas, people who are very frail and/or demented often really need these services. Some people are lucky enough to have a spouse or children who take care of them, but that can become a crushing burden. Others aren't so lucky. These services are very expensive, and will destroy most people's retirement savings in a very few years. In 2003, the average daily rate for a "semi-private" (i.e., not private) room in a nursing home in the U.S. was about $160, which is almost $60,000 a year. And these costs continue to increase faster than inflation.
Once you're broke, you qualify for Medicaid, which does pay for long-term and custodial care. So people have an incentive to give away assets to their heirs before they need long-term care, and the inheritance is destroyed. The old rules required that when someone applies for Medicaid, any assets transferred less than three years ago would be counted as though the person still had them, until three years after the transfer. The new rules impose a five-year "look back period," and the start of the waiting period now begins at the time of the application, rather than the time of the asset transfer. In other words (as I understand it, and I haven't been able to nail this down definitively so clarifications are welcome), if you gave away money to your kids five years ago, and you apply for Medicaid today, you won't be able to qualify for five years. Note that the change affects only middle class people. The poor already qualify for Medicaid, and the wealthy never will.
Now, the spectacle of moderately well-to-do seniors putting the burden of their nursing home care on taxpayers when they might have been able to pay for it themselves is unseemly to some. On the other hand, only a minority of people ever actually need expensive long-term care -- a lot of us are in decent health until a brief final illness. So there is no justice in the destruction of estates by the need for long-term care, it's just misfortune. If Medicare were to pay for it, the burden would be shared by everyone. Perhaps that is more just after all, so why shouldn't people try to arrange for justice for their own heirs?
The new rules create other problems, obviously. People often make gifts to their children without the slightest thought about one day needing nursing care. They give a down payment for a house, college education for grandchildren, etc. Now, if you do this, and then unexpectedly have a long-term illness, you may exhaust your assets and have absolutely no way to pay for your care. What then? Will nursing homes dump people in the parking lot? There seems to be no answer to that question.
Remember that this is the administration that wants to permanently repeal the "death tax," on the grounds that it is somehow immoral for people not to inherit 100% of their parents' assets. But fate imposes a death tax at random, which the administration now wants to make it essentially impossible to avoid. Does this make sense?
Wednesday, February 08, 2006
The wrong surprise
Undoubtedly by now you have been exposed to the screaming headlines in the newspapers and on the TV fake news shows (that's ABC News, CBS News, NBC News, etc.) about the astonishing new study that finds that, as the NYWT headline has it, "Low-Fat Diet Won't Stop Cancer or Heart Disease." Oh no! Now we're totally confused! This is the opposite of what they've been telling us all these years! Nobody knows anything!
Actually, no. The only thing that's surprising about this study is that they managed to get ahold of $40 million of your money to conduct such a pointless project.
In the first place, we have known for years -- for at least a decade officially, and longer than that if we were paying attention -- that the issue is not how much fat you eat, it's what kind of fat. Most kinds of vegetable oil are just fine, and olive oil is actually good for you. Ditto fish oil. (Stay away from palm oil.) If a tasty dressing encourages you to eat salad, so much the better. Pour it on! Avoid saturated fats -- mostly animal fats from meat and dairy -- and especially trans-fats, a synthetic form of fat used in mass-produced baked goods and other processed foods.
In fact, the women in this study who started out eating high amounts of saturated fat, and managed to cut down, did experience the expected health benefits. It's just that the study wasn't designed to test that. (The women on the low-fat diet only marginally increased their consumption of fruits and vegetables, by the way.)
Second, cancer and heart disease develop over decades. All of the subjects in this study were at least 50 years old when they started, and the study only ran for 8 years. Most of the women who were diagnosed with cancer or heart disease during the eight years already had it before the study even began.
So get a grip folks. Nothing has changed. There is no new information here. We are not more confused than before, or rather we wouldn't be if the journalists who cover health issues knew what the heck they were talking about. The same advice still stands. Please ignore this.
That's my story and I'm sticking to it.
Tuesday, February 07, 2006
Strictly Construct This
The right of the people to be secure in their persons, houses, papers, and effects, against unreasonable searches and seizures, shall not be violated, and no warrants shall issue, but upon probable cause, supported by oath or affirmation, and particularly describing the place to be searched, and the persons or things to be seized.
Blog prostituting . . .
To put it politely.
New post up at Critical Condition.
And don't forget to check out Zig's post at Today in Iraq, if you're interested in what goes on in the land where civilization began, but is barely holding on.
Alternatives
The subject of what is widely called Complementary and Alternative Medicine (CAM) is one in which I have long-standing interest, involvement, and experience, but have not previously discussed here, for several reasons. But yesterday's post on quackery, while not intended to address the subject of CAM per se, does oblige me to do so now.
A fundamental difficulty with all of the discussion in this area, including some of the most widely cited literature such as the surveys conducted by Harvard physicians David Eisenberg, Thomas DelBanco and colleagues* (e.g., Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States: prevalence, costs, and patterns of use. N Engl J Med. 1993;328 (4):246-252) is that nobody is quite sure what the term means. The Eisenberg surveys included such methods as chiropractic, massage therapy, meditation and even exercise regimens such as yoga among CAM modalities, but these are accepted by most medical doctors as being useful in certain circumstances or even very generally.
Drug companies routinely investigate herbs used in various traditions for efficacy, and even send expeditions to the Amazon jungle to learn from healers and bring back their remedies for study. Many of the most important pharmaceuticals are compounds derived from plants, or variations on those compounds, that were used for centuries or millenia before Merck and Pfizer came along -- NSAIDs, opiates, digitalis, you name it. Of course for many people the bad news is that the drug companies get patents on compounds and make a fortune while the shamans just get their land destroyed by loggers, but that's a separate issue.
A lot of MDs claim there is no such thing as "alternative" medicine -- that if something is found to actually work, according to standards of evidence, then so-called allopathic practitioners (for historical reasons, that's the term for people who go to accredited medical schools and get licensed to practice as M.D.s) will happily adopt it. As I said before, this isn't always entirely true, there is prejudice and resistance to radical ideas within allopathic medicine. Actually the prejudice isn't directed only at people who come from outside of the credentialed, faculty-appointed community. Stanley Prusiner's claims about prions were rejected and ridiculed for years, until they finally became accepted. But they were ultimately accepted, because the evidence was there. Homeopathy, in contrast, has not been accepted because a) trials consistently show it to be no better than placebo, and b) the proposed mechanism of action of homeopathic remedies is completely nonsensical and inconsistent with everything we know about physical reality.
However, many people derive benefit from homeopathic remedies. How can this be? We all know the answer: people often feel better, and even actually get better, when they believe that what they are doing will be helpful. And anyway, most of the symptoms that plague us get better on their own soon enough. Allopathic medicine has a tendency to do too much. Its very powerful interventions can do harm as well as good, and we are often better off leaving well enough alone and letting nature take its course. As I myself said just recently, you're better off drinking ginger tea than taking over-the-counter (or for that matter, prescription) cough and cold remedies. You're also better off taking homeopathic remedies, which are just water, and therefore will not hurt you. If it makes you feel better, who am I to object?
But the real key is that various systems of healing interact with people -- as people, not just biological systems -- in different ways. CAM practitioners as such, people who declare themselves to be non-allopathic physicians, draw on different theories of health and human nature than do allopaths. These theories lead them to ask different questions, speak with and touch people differently, than do allopathic physicians. Their practice settings are different, they may be more available, they may provide a framework of explanation which is comforting. A naturopath or ayurvedic practitioner may have some remedies within his or her kit that are biologically active and would be found efficacious in a randomized controlled trial, and others that are not. Someday those trials may be done, and some of those remedies may be adopted by allopaths.
But in the meantime, people may derive other benefits from their interactions with these practitioners, that they don't get from their M.D.s. They may feel that they are listened to better, that their healer understands what is really troubling them and addresses their emotional, social or spiritual needs better than their allopathic physicians. They may dislike the sterile, impersonal, hectic environment of the hospital and clinic. They may, quite legitimately, fear the potential adverse effects of aggressive medical intervention. They may not want to pay tens of thousands of dollars. Allopathic practitioners would do well to consider these dimensions far more than they do.
However, that is no excuse for quackery. There are a lot of charlatans out there who just want your money, and their remedies are crap. A good salesman convinces even himself of his lies, but they are lies nonetheless.
*Disclosure alert: I am acquainted with Dr. DelBanco.
Monday, February 06, 2006
The Reality Based Health Community
Quackwatch is a web site I have visited profitably for many years. Its owner is Dr. Stephen Barrett, a retired psychiatrist. It is a largely volunteer effort, which according to information on the site costs only about $7,000 a year to operate, and I've got to tell you, they get a lot done for the money. There is a mountain of resources there to explore, most of it very thoroughly researched, well written and often entertaining as well as informative.
A lot of the postings on the site are specific debunkings of various scam artists and popular pseudo-scientific beliefs. At times the writers (Dr. Barrett provides only some of the content) may err a bit on the side of orthodoxy, in my view. There is also plenty that goes on inside the realm of accepted medical practice that could benefit from the same squinty eyeball they direct at the con artists and fabulists who inhabit the untamed wilderness outside of it.
But criticizing medical orthodoxy is not their job. In recent years, there has been a growing and increasingly effective movement to do so from within, and therein lies the crucial difference between medicine and quackery -- medicine strives to be evidence based, in other words scientific, which means that skepticism is encouraged (at least officially) and old practices and ideas are regularly overturned when new evidence warrants. (Not often enough, maybe, but it happens.)
So I particularly commend some of the essays on the site that discuss the fundamental principles for establishing truth, including Distinguishing Science from Pseudoscience by Rory Coker, and Robert Novella's The Power of Coincidence. There is an awful lot there to explore.
The proximate reason for my bringing up Quackwatch now is that, in my view, quackery is no different from religious and other ideological claims about physical reality, such as creationism, denial of global warming, etc., as practiced by the current administration. It starts with a conclusion and works backward to justify it: cherry picking facts and ignoring others; relying on supposed authority rather than direct evidence; repeating supposed facts and observations even after they have been proved false; using the convenience or comfort of a conclusion as an argument for its validity; depending on rhetorical devices and psychological manipulation; claiming that lack of knowledge is proof of some arbitrary conclusion; and using scientific-sounding terminology and aping forms of scientific argument while simultaneously ignoring real scientific evidence and reasoning.
We live in a dangerous world. We need to confront our problems with clarity and rigor. That goes for international relations and environmental protection as well as our individual health and well being. We need to stop employing quack politicians as well as quack doctors.
Sunday, February 05, 2006
An Unpleasant Subject
Probably for no particular reason other than the generally tremulous state of the zeitgeist, there are a lot of rumors, speculation and theories floating around to the effect that non-state actors, presumably Jihadists of one stripe or another, already possess one or more functional nuclear weapons. That would certainly be bad news. A semi-related issue, obviously, is the question of Iran's alleged pursuit of nuclear weapons, and nuclear proliferation more generally.
It occurs to me that this is a field of the greatest public concern in which most people don't understand the basic scientific issues. I expect my readers are pretty sophisticated, but I'd like to know -- did you know all or most of what I'm about to explain, or is any of it news? (If I'm boring you with stuff you already know, you can go check out Today in Iraq, where I did the post today.)
In order to make a nuclear weapon, you need a sufficient amount of either the element plutonium -- any isotope will work, but it's easier to use material consisting predominantly of Pu239 -- or so-called highly enriched uranium (HEU). Naturally occuring uranium consists mostly of the istope U238, but you need at least 20% U235, and preferably a higher proportion, to make a bomb. For nuclear reactor fuel, you only need enrichment to 3% or so.
Plutonium is almost non-existent in nature, but it builds up in nuclear reactor fuel as it is "burned" for power. It can be extracted chemically from used fuel rods, but they are highly radioactive and dangerous to handle. It is also considerably more difficult to make a functional plutonium bomb than it is to make a bomb from HEU.
HEU has low radioactivity and can be handled without special precautions. Even worse, if you have less than 400 Kg of 20% U235, or as little as 20Kg of 90% or more U235, it is astonishingly easy to make a bomb. No high technology is needed. A nuclear explosion occurs when a sufficient mass of weapons-grade fissionable material is aggregated. To make an HEU bomb, all you need is a gun with a closed barrel. Put a lump of HEU of more than 50% critical mass in the closed end, and a similar lump in the chamber, then fire the gun. The lump in the chamber will smash into the lump at the other end, and goodbye Peoria. Such devices are so simple to build and so reliable that it is thought that a terrorist could confidently make and deploy one, even though testing would obviously be impossible.
Making a plutonium bomb requires a much more sophisticated device in which a hollow ball of plutonium is forcefully imploded. Sophisticated industrial facilities would be necessary, and a manufacturer would probably not be confident that it worked without being able to test the design.
Fortunately, it is very difficult to enrich uranium. The isotopes can only be separated by taking advantage of the difference in their atomic weights, which is tiny. Enriching uranium requires huge industrial plants with large amounts of precision machinery. It is only feasible for states.
Used nuclear fuel rods are "too hot to handle" at first, but after 25 years or so they cool down to the point where a relatively sophisticated non-state actor could conceivably extract the plutonium.
So there are three conceivable ways for a non-state actor to obtain a working nuclear weapon, without the cooperation of a state:
a) Steal an actual, working nuclear weapon from a national arsenal;
b) Steal enough HEU, and make your own bomb;
c) Either steal plutonium, or steal some decades-old used nuclear fuel rods and extract the plutonium, and then somehow obtain sophisticated design information and hardware.
At present, any scenario under (c) seems implausible. However, in the fuel-recycling/breeder reactor future proposed by the Bush administration, there will be far more used nuclear fuel and plutonium in circulation. Used reactor fuel also makes a fabulous "dirty bomb," so there will be very serious security concerns with any such nuclear economy.
The HEU scenario, unfortunately, is more plausible. After the collapse of the Soviet Union, many security guards and scientists at nuclear weapon and research sites went unpaid and facilities were left unsecured. An engineer at one facility actually did steal 1.5 Kg of HEU, hoping to sell it for profit. He was caught, but nobody can rule out that other thefts were not thwarted. Since 1993, U.S.-Russian cooperation has resulted in great improvements in the security of former soviet nuclear sites, but it's hard to know how good security really is presently. There are also substantial stockpiles of HEU in Kazakhstan, Uzbekistan, Belarus, Ukraine, and other places whose political stability and national security competence may be uncertain.
As for someone stealing an intact weapon, most U.S. and Soviet/Russian weapons have fail-safe devices that make them impossible to detonate without access to security codes. (I'm not sure why it wouldn't be possible to extract HEU from a device and build your own detonator for it, but evidently they are booby-trapped to make this extremely difficult.) However, so-called tactical (i.e., comparatively small) nuclear weapons in the former Soviet arsenal have been reported to lack these fail-safe devices. The Russians claim that all Soviet weapons are accounted for, but it's impossible to know if they are telling the truth, or even whether they really know.
The bottom line is, it seems unlikely, but it is not impossible, that there are one or more loose nukes out there somewhere. If so, they are bulky -- the idea of a "suitcase bomb" is unrealistic, we're talking something more like a steamer trunk, at least. You can't smuggle it in your checked luggage, but you could ship it.
What to do? Collect as much HEU as possible, from military and research sites around the world. Dilute it with U238. Then it can be used as reactor fuel. Think twice and three times about a future plutonium economy. Stop further nuclear weapons proliferation, but that can only happen if the present nuclear powers get serious about disarmament. Why should Iran or other regional powers agree to give up uranium enrichment and the prospect of acquiring nuclear weapons if it's perfectly alright for Israel, Pakistan, India, the U.S., Russia, China, France and the UK to have them? Obviously they won't and there isn't any moral case to be made why they should.
The human and political consequences of any sort of attack using a nuclear explosive weapon, anywhere, are incalculable. One can easily think of some prospects that are far too painful to contemplate. The one thing that Kerry and Bush agreed on in their "debates" was that this is what worries them the most. But Mr. Bush hasn't actually done anything about it, because it requires diplomacy, international cooperation, and humility on the part of the United States, not bullying and U.S. exceptionalism.
Friday, February 03, 2006
The "H" Word
A few people took exception to a recent post of mine in which I compared the U.S.A. today (the country, not the newspaper) to Germany in the 1930s. It seems that people object strenuously to comparing any human being, in any way, to Adolf Hitler. To do so is to trivialize Mr. Hitler's supposedly unprecedented, unapproachable, incomparable, all time number 1 evilness, and anyone who makes such a comparison is a Holocaust denier, or something like that. Of course I didn't actually compare anyone to Hitler, except perhaps by implication, but even inviting people to make their own comparisons turns out to be politically incorrect. Who knew?
So anyhow, the SecDef now compares Venezuelan president Hugo Chavez to Adolf Hitler, and not just by suggestion. Unlike certain other world leaders, Mr. Chavez, as far as I know, has never tortured anyone, never started any unprovoked wars of aggression, and is not responsible for the deaths of millions or hundreds of thousands or even one human being. The basis for Mr. Rumsfeld's comparison, as far as Rumsfeld has explained himself, is that both Hitler and Chavez were elected legally: “I mean, we’ve got Chavez in Venezuela with a lot of oil money. He’s a person who was elected legally — just as Adolf Hitler was elected legally — and then consolidated power and now is, of course, working closely with Fidel Castro and Mr. Morales and others.” So I guess that lets Mr. Rumsfeld's boss off the hook.
(It is news to me that Hitler worked closely with Evo Morales and Fidel Castro, but live and learn. If you follow the link, MSNBC will let you vote on whether the comparison was appropriate.)
Why do I not have faith . . .
in faith based substance abuse treatment? As I believe I have mentioned here before, the Substance Abuse and Mental Health Services Administration is working and praying to steer more of your tax dollars to "faith based" providers of substance abuse treatment, through its Center for Substance Abuse Treatment (CSAT).
One minor obstacle is that churches don't, as a general rule, have any expertise, training, or least clue about how to actually treat substance abuse. So, CSAT is investing your tax dollars in training and technical assistance for churches that want to apply for CSAT funding. Naturally, the first thing you need to be able to do if you want to get funding is write a proposal, so that's what the training and technical assistance is all about.
Okay, so let's say you're the Rock of Ages Fire Baptized Church of God in Jesus Christ, Christian, and you go to the workshop and learn how to write a really good proposal, and you get the money. Then what do you do?
Here's an idea you can steal from Central Christ Church of Salt Lake City, Utah, which forced clients who were court ordered into treatment to work as telemarketers for 28 cents an hour. The proceeds went into church coffers. Now that's one way to fight for the Christian dominion!
(As far as I can determine Central Christ Church does not, at least as yet, have CSAT funding, not directly. But if it had state funding, as it apparently did, it was supported at least in part by Utah's formula grant. Presumably the state of Utah has felt encouraged to contract with "faith based" providers by the federal initiative.)
Thursday, February 02, 2006
They never stop thinking up new ways to screw us
On this day that shall live in infamy -- the day that God told George W. Bush to sign a bill that got through the Senate thanks to a tie-breaking vote by President Cheney, and got through the house by two votes with arms twisted out of their sockets littering the house floor, the bill that will force working poor people off of Medicaid and make the ones who are left pay money they don't have for doctor visits and pills -- I have come across yet another outrage.
The FDA has recently revised labelling requirements for medications. Good idea, they are now somewhat more stringent. On page 169 of the new rule, which you can read here if you're willing to wait 5 minutes for the PDF to load and then scroll down (it's page 75 of the PDF file, since the document is broken into multiple files), you will read the following:
X. Executive Order 13132: Federalism
We have analyzed this final rule in accordance with the principles set forth in Executive Order 13132. Section #a) of the Executive order requires agencies to “construe * * * a Federal statute to preempt State law only where the statute contains an express preemption provision or there is some other clear evidence that the Congress intended preemption of State law, or where the exercise of State authority conflicts with the exercise of Federal authority under the Federal statute.“ Here, FDA has determined that the exercise of State authority conflicts with the exercise of Federal authority under the act.
What this means in English is that it will be harder for people to sue drug manufacturers. It means that the FDA says that if manufacturers comply with the labelling requirements, they can't be sued under state law for failing to warn people about adverse effects. (State courts don't have to agree with them, but it puts a thumb on the scale.) Here's what Public Citizen has to say about this. Excerpt:
In a further blow to consumers, the final rule now contains a preamble aimed at preempting the rights of patients to sue drug manufacturers if a drug is approved by the FDA. The Bush administration has previously failed to persuade Congress and, with a few exceptions, the courts (where it has filed amicus briefs) to shield drug makers from liability. The new tactic of writing preemption language into federal regulation notices is an attempt to bypass Congress and override consumer protection liability laws, said Public Citizen President Joan Claybrook. The administration has also used such language in recently proposed automobile safety rules.
“This is a sneak attack on consumer rights,” Claybrook said. “President Bush is once again abusing his executive powers, this time in his attempt to protect the big pharmaceutical companies from the consequences of their actions. Thousands of people in this country have died or been seriously injured by drugs approved by the FDA, and this administration is saying it doesn’t think people should have any recourse.”
And here's what I have to say. I want an FDA that works to protect the people, not to protect the drug companies. I want a federal government that respects the rights of the states and the people. I want a government that isn't run by hypocrites, liars, thieves and, oh yeah, murderers. That's what I want. It's the Christian thing to ask.
Wednesday, February 01, 2006
Is a human-chimpanzee hybrid morally repugnant?
On doctor's orders, I didn't watch, but I understand that one of the bold new initiatives put forth last night was something like, "Tonight I ask you to pass legislation to prohibit the most egregious abuses of medical research – human cloning in all its forms … creating or implanting embryos for experiments … creating human-animal hybrids …"
Technically speaking, as far as we know, a human-animal "hybrid" per se is not possible. Hybridization requires that two species be mutually fertile. For example a mule is a (sterile) hybrid of an ass and a mare. Lions and tigers, believe it or not, can interbreed, as can anise and dill. But the Great Moralist was talking about other possibilities, even if he didn't understand what he was saying.
Cloning, as such, really comes into this only in a very limited way. The method which has been used to clone sheep and other mammals is called Somatic Cell Nuclear Transplant, in which the nucleus from a cell of one animal -- just about any old cell, such as a skin cell -- is placed into an ovum from which the nucleus has been removed. This chimeric cell may then start to behave like a normally fertilized ovum, and develop into an embryo. The nucleus contains more than 99% of a cell's genetic material, including all of the genes which guide development, hence the new creature will be nearly identical to the one from which the nucleus was taken. However, the cells of people and all multicellular organisms, called eukaryotic cells, contain endosymbionts -- the descendants of ancient bacteria, called mitochondria, which are essential to cellular metabolism, and have their own DNA. Hence if you were to put a human nucleus into, say, a denucleated cow ovum, and get it to develop, you would get a human being in every respect, except for its mitochondrial DNA. You wouldn't be able to tell that there was anything unusual about the person unless you were to sequence its mitochondrial DNA (assuming that there wasn't some metabolic disorder associated with the situation, which is unknown).
There are other ways of combining human and animal genes in one being. One which is being actively pursued is xenotransplantation. If organs from, say, pigs, could be modified so that they did not provoke an immune response from humans, they would be available for transplant. That has actually been tried, by doctors who unsuccessfully transplanted a baboon's heart into a baby. This was widely considered unethical, but only because the experiment had little chance of success and only added to the baby's suffering. No doubt if it had worked it would be done all the time now, and people would view it as a method of saving lives, not a moral abomination.
Another kind of experiment, which has been done, is to grow specific human tissues within animals. For example, human cancer cells can be made to grow in mice, to test theories about cancer or to test treatments. Yet another procedure, which is now done routinely, puts single genes that code for a specific protein into a foreign species. For example, genes for human hormones have been introduced into goats, so that the hormone can be extracted from the goats' milk for medicinal purposes.
A morally more questionable procedure is to add one or more embryonic stem cells from species A to an embryo of species B. If such an embryo is viable, what will probably happen is that it will follow the developmental pathway it has already established, in other words develop into animal A, but the adult animal will have cells of the other species interspersed throughout its tissues. Who knows what, if any, gross abnormalities might be associated with this situation?
Then there is the science fiction scenario, well outside the present capabilities of science, of using genetic engineering techniques to equip humans with attributes of other species, such as wings or gills.
Note that only the first of these techniques necessarily involves cloning, and that some of them appear to be morally troubling but others do not. The American Journal of Bioethics did a major consideration of "crossing species boundaries" in 2003, with a lead essay by Jason Scott Robert and Francoise Baylis. There are nearly two dozen responses, which may be a bit much, but I recommend reading at least a couple to get a flavor of how these issues are debated.
Robert and Baylis point out that defining the boundaries among species is quite uncertain. While humans are biologically distinguishable, it is not at all settled what characteristics give an entity the moral status of a person. Most ethical arguments against creating any sort of part human creature are not very convincing, but they find the most convincing one is simply the confusion it would cause. Presently we have an unexamined, "folk" consensus that humans are morally distinct entities, and it just seems dangerous to start muddying the waters too much.
Frankly, I don't see the waters muddied by, say, a person with a transplanted pig's liver, or a laboratory animal that includes some human cells or tissues for purposes of medical research. (Animal rights advocates will be offended, but that is a separate issue and certainly not the concern behind the SOTU admonition.)
What do you think?